

Obstructive sleep apnoea during REM sleep and incident non-dipping of nocturnal blood pressure: a longitudinal analysis of the Wisconsin Sleep Cohort
- PMID: 26307037
- PMCID: PMC7888359
- DOI: 10.1136/thoraxjnl-2015-207231
Obstructive sleep apnoea during REM sleep and incident non-dipping of nocturnal blood pressure: a longitudinal analysis of the Wisconsin Sleep Cohort
Abstract
Background: Non-dipping of nocturnal blood pressure (BP) is associated with target organ damage and cardiovascular disease. Obstructive sleep apnoea (OSA) is associated with incident non-dipping. However, the relationship between disordered breathing during rapid eye movement (REM) sleep and the risk of developing non-dipping has not been examined. This study investigates whether OSA during REM sleep is associated with incident non-dipping.
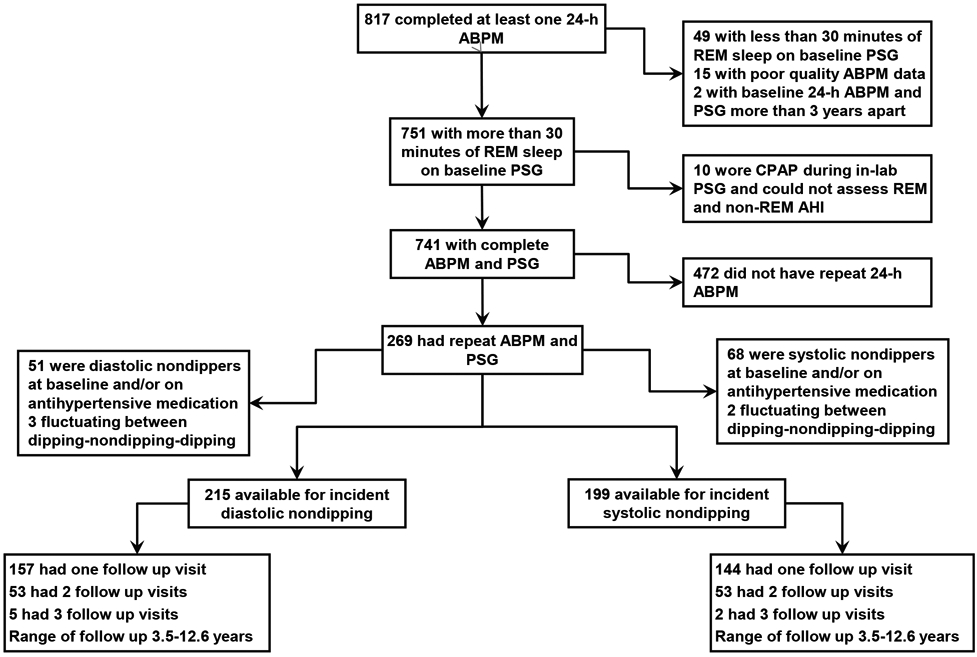
Methods: Our sample included 269 adults enrolled in the Wisconsin Sleep Cohort Study who completed two or more 24 h ambulatory BP studies over an average of 6.6 years of follow-up. After excluding participants with prevalent non-dipping BP or antihypertensive use at baseline, there were 199 and 215 participants available for longitudinal analysis of systolic and diastolic non-dipping, respectively. OSA in REM and non-REM sleep were defined by apnoea hypopnoea index (AHI) from baseline in-laboratory polysomnograms. Systolic and diastolic non-dipping were defined by systolic and diastolic sleep/wake BP ratios >0.9. Modified Poisson regression models estimated the relative risks for the relationship between REM AHI and incident non-dipping, adjusting for non-REM AHI and other covariates.
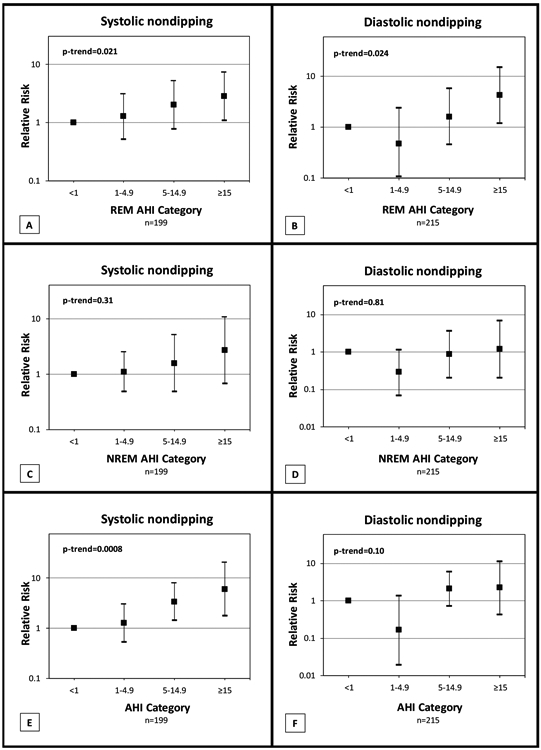
Results: There was a dose-response greater risk of developing systolic and diastolic non-dipping BP with greater severity of OSA in REM sleep (p-trend=0.021 for systolic and 0.024 for diastolic non-dipping). Relative to those with REM AHI<1 event/h, those with REM AHI≥15 had higher relative risk of incident systolic non-dipping (2.84, 95% CI 1.10 to 7.29) and incident diastolic non-dipping (4.27, 95% CI 1.20 to 15.13).
Conclusions: Our findings indicate that in a population-based sample, REM OSA is independently associated with incident non-dipping of BP.
Keywords: Sleep apnoea.
Published by the BMJ Publishing Group Limited. For permission to use (where not already granted under a licence) please go to http://group.bmj.com/group/rights-licensing/permissions.
Figures
References
-
- Pickering TG, White WB, Giles TD, et al. When and how to use self (home) and ambulatory blood pressure monitoring. J Am Soc Hypertens 2010; 4:56–61 - PubMed
-
- Pickering TG, Shimbo D, Haas D. Ambulatory blood-pressure monitoring. N Engl J Med 2006; 354:2368–2374 - PubMed
-
- Dolan E, Stanton A, Thijs L, et al. Superiority of ambulatory over clinic blood pressure measurement in predicting mortality: the Dublin outcome study. Hypertension 2005; 46:156–161 - PubMed
-
- Chobanian AV, Bakris GL, Black HR, et al. The Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure: the JNC 7 report. JAMA 2003; 289:2560–2572 - PubMed
-
- Staessen JA, Thijs L, Fagard R, et al. Predicting cardiovascular risk using conventional vs ambulatory blood pressure in older patients with systolic hypertension. Systolic Hypertension in Europe Trial Investigators. JAMA 1999; 282:539–546 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical