

Comparison of physical interventions, behavioral interventions, natural health products, and pharmacologics to manage hot flashes in patients with breast or prostate cancer: protocol for a systematic review incorporating network meta-analyses
- PMID: 26307105
- PMCID: PMC4549873
- DOI: 10.1186/s13643-015-0099-y
Comparison of physical interventions, behavioral interventions, natural health products, and pharmacologics to manage hot flashes in patients with breast or prostate cancer: protocol for a systematic review incorporating network meta-analyses
Abstract
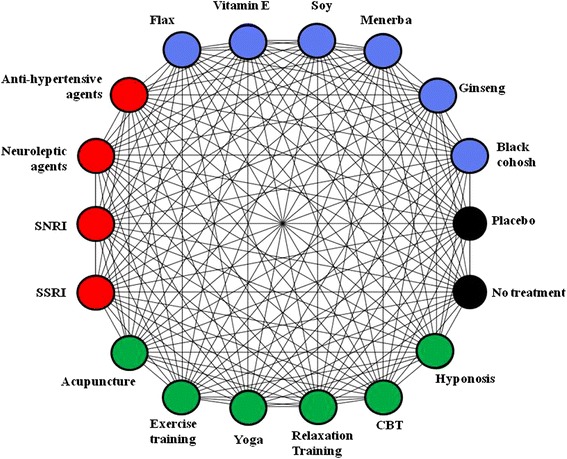
Background: Breast and prostate cancers are the most commonly diagnosed non-dermatologic malignancies in Canada. Agents including endocrine therapies (e.g., aromatase inhibitors, gonadotrophin-releasing hormone analogs, anti-androgens, tamoxifen) and chemotherapy have improved survival for both conditions. As endocrine manipulation is a mainstay of treatment, it is not surprising that hot flashes are a common and troublesome adverse effect. Hot flashes can cause chills, night sweats, anxiety, and insomnia, lessening patients' quality of life. These symptoms impact treatment adherence, worsening prognosis. While short-term estrogen replacement therapy is frequently used to manage hot flashes in healthy menopausal women, its use is contraindicated in breast cancer. Similarly, testosterone replacement therapy is contraindicated in prostate cancer. It is therefore not surprising that non-hormonal pharmacological treatments (anti-depressants, anti-epilectics, anti-hypertensives), physical/behavioral treatments (e.g., acupuncture, yoga/exercise, relaxation techniques, cognitive behavioral therapy), and natural health products (e.g., black cohosh, flax, vitamin E, ginseng) have been studied for control of hot flashes. There is a need to identify which interventions minimize the frequency and severity of hot flashes and their impact on quality of life. This systematic review and network meta-analysis of randomized studies will synthesize available evidence addressing this knowledge gap.
Methods/design: An electronic search of Medline, Embase, AMED, PsycINFO, and the Cochrane Register of Controlled Trials has been designed by an information specialist and peer reviewed by a second information specialist. Study selection and data collection will be performed by two reviewers independently. Risk of bias assessments will be completed using the Cochrane Risk of Bias Scale. Outcomes of interest will include validated measures of hot flash severity, hot flash frequency, quality of life, and harms. Bayesian network meta-analyses will be performed where judged appropriate based on review of clinical and methodologic features of included studies.
Discussion: Our review will include a broad range of interventions that patients with breast and prostate cancer have attempted to use to manage hot flashes. Our work will establish the extent of evidence underlying these interventions and will employ an inclusive approach to analysis to inform comparisons between them. Our findings will be shared with Cancer Care Ontario for consideration in the development of guidance related to supportive care in these patients.
Prospero: CRD42015024286.
Figures
Similar articles
-
Complementary/alternative therapies for reducing hot flashes in prostate cancer patients: reevaluating the existing indirect data from studies of breast cancer and postmenopausal women.Urology. 2002 Apr;59(4 Suppl 1):20-33. doi: 10.1016/s0090-4295(02)01641-2. Urology. 2002. PMID: 11937433 Review.
-
ONS Guidelines™ for Cancer Treatment-Related Hot Flashes in Women With Breast Cancer and Men With Prostate Cancer.Oncol Nurs Forum. 2020 Jul 1;47(4):374-399. doi: 10.1188/20.ONF.374-399. Oncol Nurs Forum. 2020. PMID: 32555554
-
The maintenance effect of acupuncture on the side effects of breast cancer endocrine therapy: A protocol for systematic review and meta analysis.Medicine (Baltimore). 2020 Jun 12;99(24):e20567. doi: 10.1097/MD.0000000000020567. Medicine (Baltimore). 2020. PMID: 32541483 Free PMC article.
-
Complementary and alternative medicine for menopausal symptoms: a review of randomized, controlled trials.Ann Intern Med. 2002 Nov 19;137(10):805-13. doi: 10.7326/0003-4819-137-10-200211190-00009. Ann Intern Med. 2002. PMID: 12435217 Review.
-
The future of Cochrane Neonatal.Early Hum Dev. 2020 Nov;150:105191. doi: 10.1016/j.earlhumdev.2020.105191. Epub 2020 Sep 12. Early Hum Dev. 2020. PMID: 33036834
Cited by
-
Biobehavioral effects of Tai Chi Qigong in men with prostate cancer: Study design of a three-arm randomized clinical trial.Contemp Clin Trials Commun. 2019 Aug 21;16:100431. doi: 10.1016/j.conctc.2019.100431. eCollection 2019 Dec. Contemp Clin Trials Commun. 2019. PMID: 31650067 Free PMC article.
-
The pharmacological and non-pharmacological treatment of attention deficit hyperactivity disorder in children and adolescents: A systematic review with network meta-analyses of randomised trials.PLoS One. 2017 Jul 12;12(7):e0180355. doi: 10.1371/journal.pone.0180355. eCollection 2017. PLoS One. 2017. PMID: 28700715 Free PMC article.
-
An evaluation of DistillerSR's machine learning-based prioritization tool for title/abstract screening - impact on reviewer-relevant outcomes.BMC Med Res Methodol. 2020 Oct 15;20(1):256. doi: 10.1186/s12874-020-01129-1. BMC Med Res Methodol. 2020. PMID: 33059590 Free PMC article.
-
Effects of Integrated Chinese Traditional Medicine and Conventional Western Medicine on the Quality of Life of Breast Cancer Patients: A Systematic Review and Meta-Analysis.Evid Based Complement Alternat Med. 2022 Jan 7;2022:3123878. doi: 10.1155/2022/3123878. eCollection 2022. Evid Based Complement Alternat Med. 2022. PMID: 35035500 Free PMC article.
-
[Androgen deprivation therapy of prostate cancer from a geriatric perspective].Z Gerontol Geriatr. 2025 Jul;58(4):324-335. doi: 10.1007/s00391-025-02454-0. Epub 2025 Jun 23. Z Gerontol Geriatr. 2025. PMID: 40549200 Review. German.
References
-
- Canadian Cancer Society. Prostate Cancer Statistics. http://www.cancer.ca/en/cancer-information/cancer-type/prostate/statisti.... Accessed on September 15, 2014.
-
- Canadian Breast Cancer Foundation. Breast Cancer in Canada, 2013. 2014 http://www.cbcf.org/ontario/AboutBreastCancerMain/FactsStats/Pages/Breas....
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
