

Who Must We Target Now to Minimize Future Cardiovascular Events and Total Mortality?: Lessons From the Surveillance, Prevention and Management of Diabetes Mellitus (SUPREME-DM) Cohort Study
- PMID: 26307132
- PMCID: PMC4703450
- DOI: 10.1161/CIRCOUTCOMES.115.001717
Who Must We Target Now to Minimize Future Cardiovascular Events and Total Mortality?: Lessons From the Surveillance, Prevention and Management of Diabetes Mellitus (SUPREME-DM) Cohort Study
Abstract
Background: Examining trends in cardiovascular events and mortality in US health systems can guide the design of targeted clinical and public health strategies to reduce cardiovascular events and mortality rates.
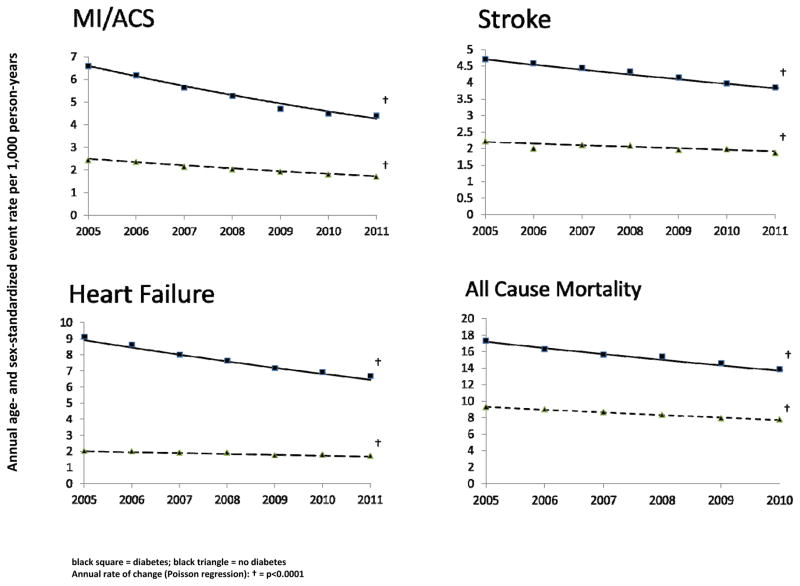
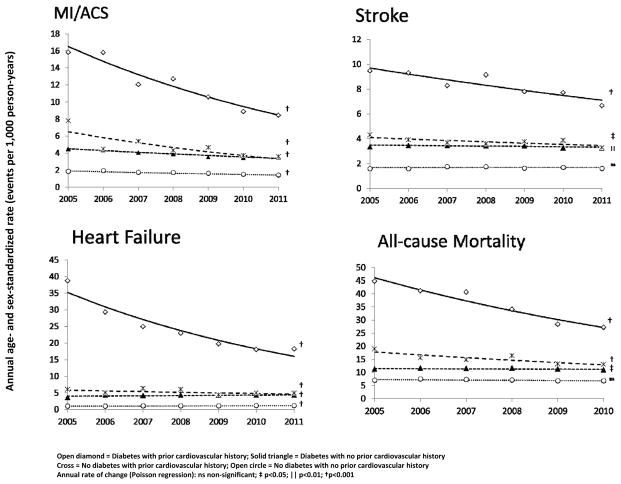
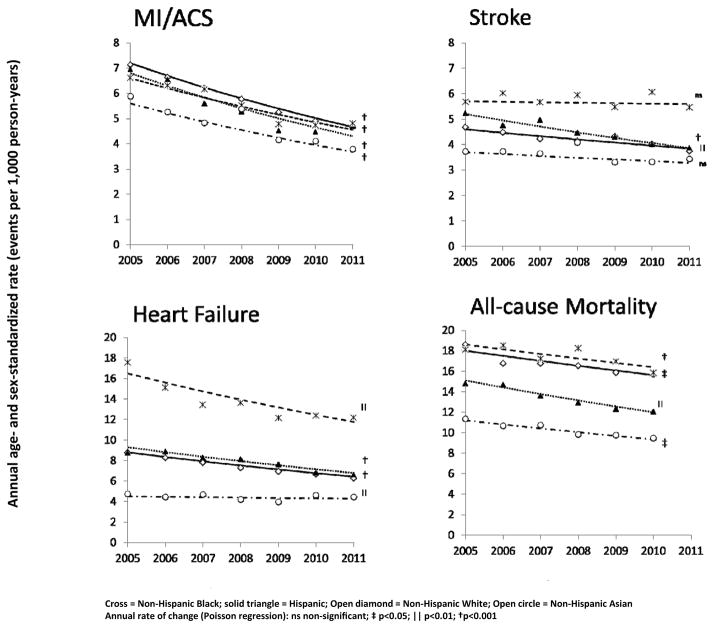
Methods and results: We conducted an observational cohort study from 2005 to 2011 among 1.25 million diabetic subjects and 1.25 million nondiabetic subjects from 11 health systems that participate in the Surveillance, Prevention and Management of Diabetes Mellitus (SUPREME-DM) DataLink. Annual rates (per 1000 person-years) of myocardial infarction/acute coronary syndrome (International Classification of Diseases-Ninth Revision, 410.0–410.91, 411.1–411.8), stroke (International Classification of Diseases-Ninth Revision, 430–432.9, 433–434.9), heart failure (International Classification of Diseases-Ninth Revision, 428–428.9), and all-cause mortality were monitored by diabetes mellitus (DM) status, age, sex, race/ethnicity, and a prior cardiovascular history. We observed significant declines in cardiovascular events and mortality rates in subjects with and without DM. However, there was substantial variation by age, sex, race/ethnicity, and prior cardiovascular history. Mortality declined from 44.7 to 27.1 (P<0.0001) for those with DM and cardiovascular disease (CVD), from 11.2 to 10.9 (P=0.03) for those with DM only, and from 18.9 to 13.0 (P<0.0001) for those with CVD only. Yet, in the [almost equal to]85% of subjects with neither DM nor CVD, overall mortality (7.0 to 6.8; P=0.10) and stroke rates (1.6–1.6; P=0.77) did not decline and heart failure rates increased (0.9–1.15; P=0.0005).
Conclusions: To sustain improvements in myocardial infarction, stroke, heart failure, and mortality, health systems that have successfully focused on care improvement in high-risk adults with DM or CVD must broaden their improvement strategies to target lower risk adults who have not yet developed DM or CVD.
Conflict of interest statement
The authors declare that they have no other relevant financial interests.
Figures
References
-
- Gregg EW, Li Y, Wang J, Burrows NR, Ali MK, Rolka D, Williams DE, Geiss L. Changes in diabetes-related complications in the United States, 1990–2010. N Engl J Med. 2014;370:1514–23. - PubMed
-
- Go AS, Mozaffarian D, Roger VL, Benjamin EJ, Berry JD, Borden WB, Bravata DM, Dai S, Ford ES, Fox CS, Franco S, Fullerton HJ, Gillespie C, Hailpern SM, Heit JA, Howard VJ, Huffman MD, Kissela BM, Kittner SJ, Lackland DT, Lichtman JH, Lisabeth LD, Magid D, Marcus GM, Marelli A, Matchar DB, McGuire DK, Mohler ER, Moy CS, Mussolino ME, Nichol G, Paynter NP, Schreiner PJ, Sorlie PD, Stein J, Turan TN, Virani SS, Wong ND, Woo D, Turner MB American Heart Association Statistics Committee and Stroke Statistics Subcommittee. Heart disease and stroke statistics--2013 update: a report from the American Heart Association. Circulation. 2013;127:e6–e245. - PMC - PubMed
-
- Bulugahapitiya U, Siyambalapitiya S, Sithole J, Idris I. Is diabetes a coronary risk equivalent? Systematic review and meta-analysis. Diabet Med. 2009;26:142–8. - PubMed
-
- Yeh RW, Sidney S, Chandra M, Sorel M, Selby JV, Go AS. Population trends in the incidence and outcomes of acute myocardial infarction. N Engl J Med. 2010;362:2155–65. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
