

Long-term risk of radionecrosis and imaging changes after stereotactic radiosurgery for brain metastases
- PMID: 26307446
- PMCID: PMC4726630
- DOI: 10.1007/s11060-015-1881-3
Long-term risk of radionecrosis and imaging changes after stereotactic radiosurgery for brain metastases
Abstract
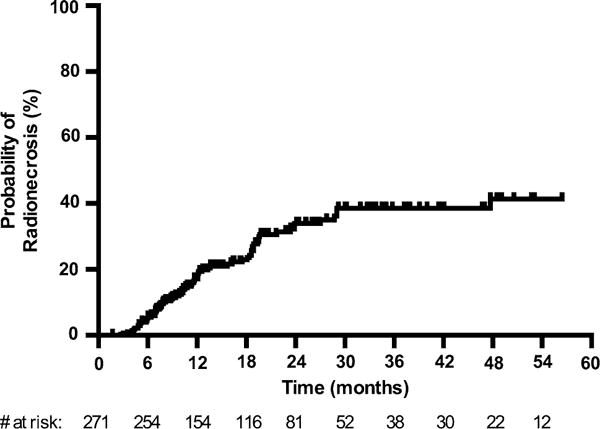
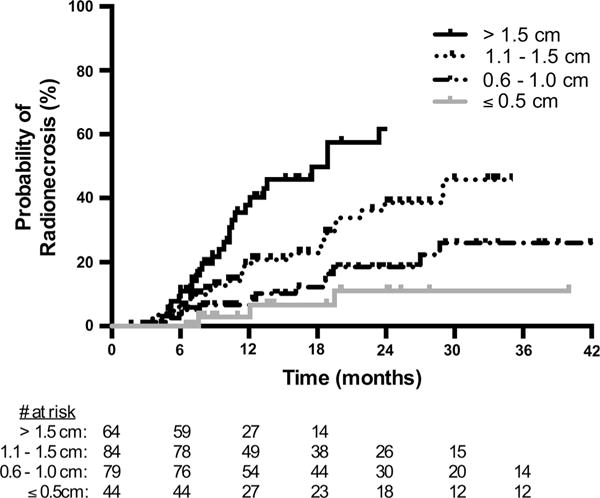
Radionecrosis is a well-characterized effect of stereotactic radiosurgery (SRS) and is occasionally associated with serious neurologic sequelae. Here, we investigated the incidence of and clinical variables associated with the development of radionecrosis and related radiographic changes after SRS for brain metastases in a cohort of patients with long-term follow up. 271 brain metastases treated with single-fraction linear accelerator-based SRS were analyzed. Radionecrosis was diagnosed either pathologically or radiographically. Univariate and multivariate Cox regression was performed to determine the association between radionecrosis and clinical factors available prior to treatment planning. After median follow up of 17.2 months, radionecrosis was observed in 70 (25.8%) lesions, including 47 (17.3%) symptomatic cases. 22 of 70 cases (31.4%) were diagnosed pathologically and 48 (68.6%) were diagnosed radiographically. The actuarial incidence of radionecrosis was 5.2% at 6 months, 17.2% at 12 months and 34.0% at 24 months. On univariate analysis, radionecrosis was associated with maximum tumor diameter (HR 3.55, p < 0.001), prior whole brain radiotherapy (HR 2.21, p = 0.004), prescription dose (HR 0.56, p = 0.02) and histology other than non-small cell lung, breast or melanoma (HR 1.85, p = 0.04). On multivariate analysis, only maximum tumor diameter (HR 3.10, p < 0.001) was associated with radionecrosis risk. This data demonstrates that with close imaging follow-up, radionecrosis after single-fraction SRS for brain metastases is not uncommon. Maximum tumor diameter on pre-treatment MR imaging can provide a reliable estimate of radionecrosis risk prior to treatment planning, with the greatest risk among tumors measuring >1 cm.
Keywords: Brain; Metastasis; Necrosis; Radionecrosis; Radiosurgery; SRS.
Conflict of interest statement
The authors declare that they have no conflicts of interest.
Figures
References
-
- Kocher M, Soffietti R, Abacioglu U, Villa S, Fauchon F, Baumert BG, Fariselli L, Tzuk-Shina T, Kortmann RD, Carrie C, Ben Hassel M, Kouri M, Valeinis E, van den Berge D, Collette S, Collette L, Mueller RP. Adjuvant whole-brain radiotherapy versus observation after radiosurgery or surgical resection of one to three cerebral metastases: results of the EORTC 22952-26001 study. J Clin Oncol. 2011;29:134–141. doi: 10.1200/JCO.2010.30.1655. - DOI - PMC - PubMed
-
- Aoyama H, Shirato H, Tago M, Nakagawa K, Toyoda T, Hatano K, Kenjyo M, Oya N, Hirota S, Shioura H, Kunieda E, Inomata T, Hayakawa K, Katoh N, Kobashi G. Stereotactic radiosurgery plus whole-brain radiation therapy vs stereotactic radiosurgery alone for treatment of brain metastases: a randomized controlled trial. JAMA, J Am Med Assoc. 2006;295:2483–2491. doi: 10.1001/jama.295.21.2483. - DOI - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
