

Outcomes after emergency abdominal surgery in patients with advanced cancer: Opportunities to reduce complications and improve palliative care
- PMID: 26307872
- PMCID: PMC4552078
- DOI: 10.1097/TA.0000000000000764
Outcomes after emergency abdominal surgery in patients with advanced cancer: Opportunities to reduce complications and improve palliative care
Abstract
Background: There is increasing emphasis on the appropriateness and quality of acute surgical care for patients with serious illness and at the end of life. However, there is a lack of evidence regarding outcomes after emergent major abdominal surgery among patients with advanced cancer to guide treatment decisions. This analysis sought to characterize adverse outcomes (mortality, complications, institutional discharge) and to identify factors independently associated with 30-day mortality among patients with disseminated cancer who undergo emergent abdominal surgery for intestinal obstruction or perforation.
Methods: This is a retrospective cohort study of 875 disseminated cancer patients undergoing emergency surgery for perforation (n = 499) or obstruction (n = 376) at hospitals participating in the American College of Surgeons' National Surgical Quality Improvement Program from 2005 to 2012. Predictors of 30-day mortality were identified using multivariate logistic regression.
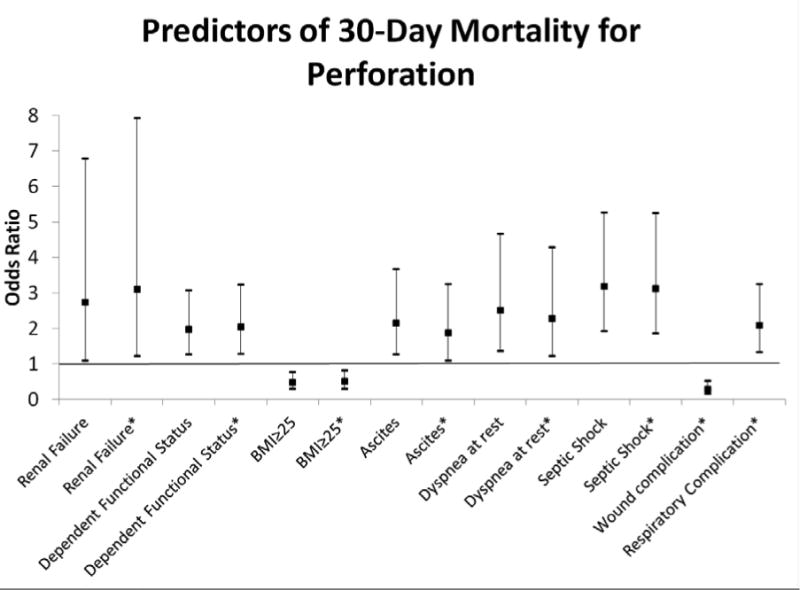
Results: Among patients who underwent surgery for perforation, 30-day mortality was 34%, 67% had complications, and 52% were discharged to an institution. Renal failure, septic shock, ascites, dyspnea at rest, and dependent functional status were independent preoperative predictors of death at 30 days. When complications were considered, postoperative respiratory complications and age (75-84 years) were also predictors of mortality.Patients who had surgery for obstruction had a 30-day mortality rate of 18% (n = 68), 41% had complications, and 60% were discharged to an institution. Dependent functional status and ascites were independent predictors of death at 30 days. In addition to these predictors, postoperative predictors of mortality included respiratory and cardiac complications. Few patients (4%) had do-not-resuscitate orders before surgery.
Conclusion: Emergency abdominal operations in patients with disseminated cancer are highly morbid, and many patients die soon after surgery. High rates of complications and low rates of preexisting do-not-resuscitate orders highlight the need for targeted interventions to reduce complications and integrate palliative approaches into the care of these patients.
Level of evidence: Prognostic study, level III; therapeutic study, level IV.
Conflict of interest statement
Figures

References
-
- Medicine Io. Washington, DC: The National Academies Press; 2014. Dying in America: Improving Quality and Honoring Individual Preferences Near the End of Life; p. 630. - PubMed
-
- Kwok AC, Semel ME, Lipsitz SR, Bader AM, Barnato AE, Gawande AA, et al. The intensity and variation of surgical care at the end of life: a retrospective cohort study. Lancet. 2011 Oct 15;378(9800):1408–13. - PubMed
-
- Cooper Z, Courtwright A, Karlage A, Gawande A, Block S. Pitfalls in Communication That Lead to Nonbeneficial Emergency Surgery in Elderly Patients With Serious Illness: Description of the Problem and Elements of a Solution. Ann Surg. 2014 May 23; - PubMed
-
- Wallston KA, Burger C, Smith RA, Baugher RJ. Comparing the quality of death for hospice and non-hospice cancer patients. Medical care. 1988 Feb;26(2):177–82. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
