

Hypoperfusion of the Adventitial Vasa Vasorum Develops an Abdominal Aortic Aneurysm
- PMID: 26308526
- PMCID: PMC4550325
- DOI: 10.1371/journal.pone.0134386
Hypoperfusion of the Adventitial Vasa Vasorum Develops an Abdominal Aortic Aneurysm
Abstract
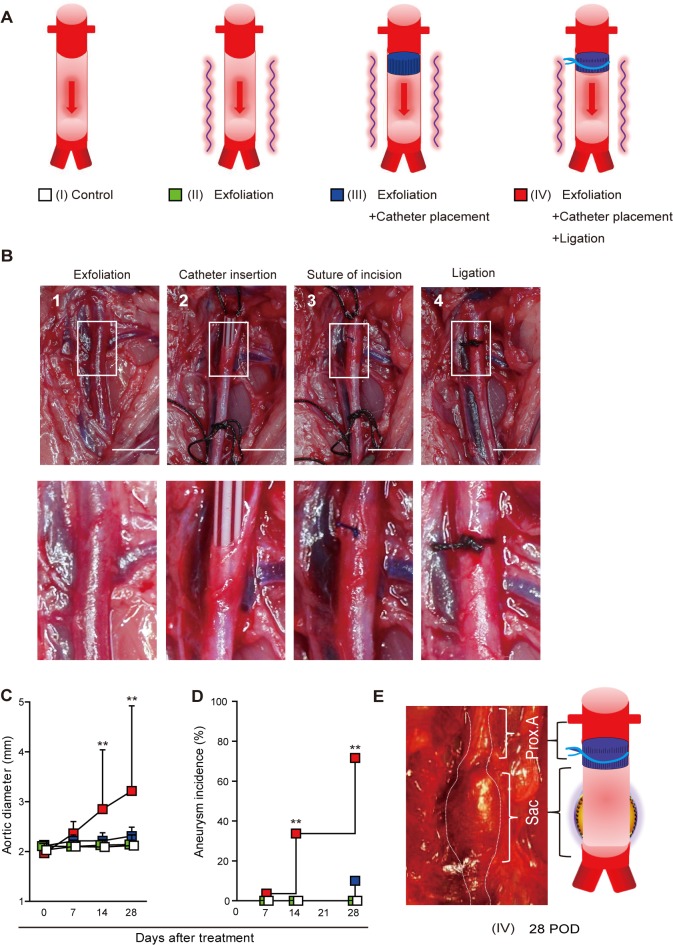
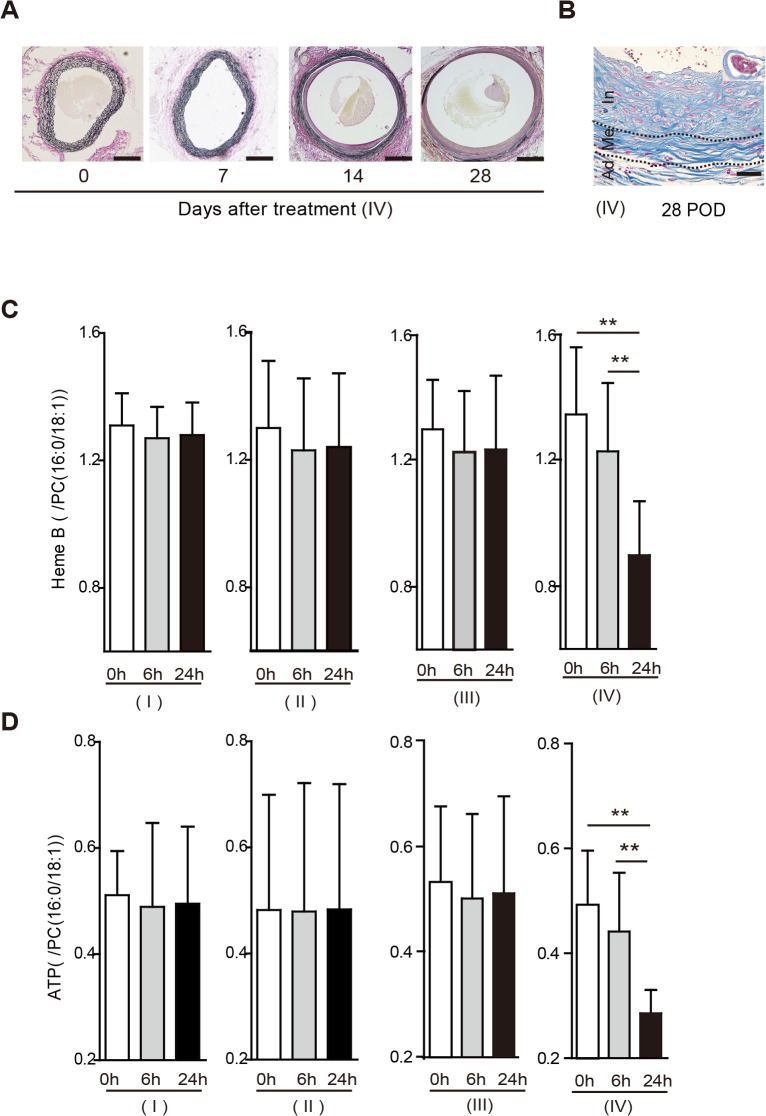
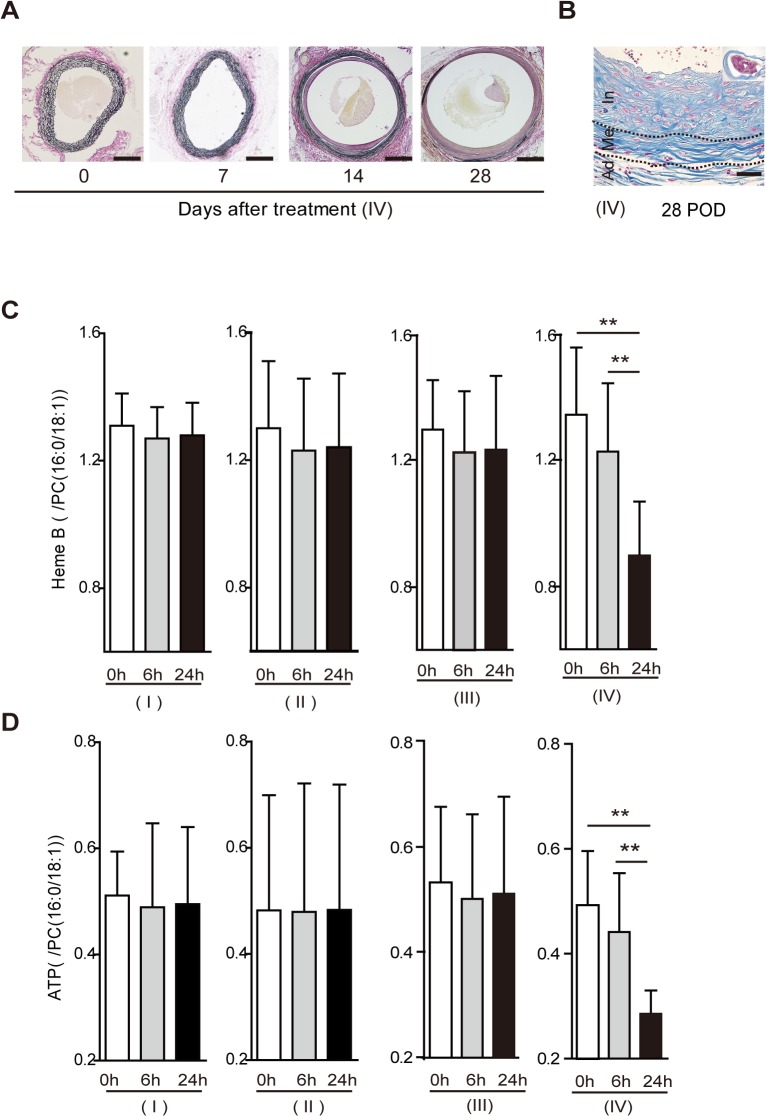
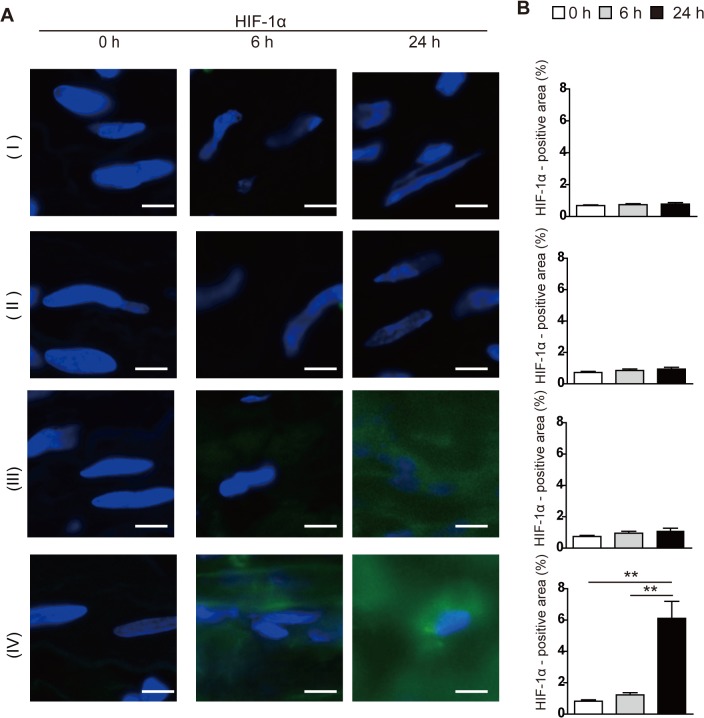
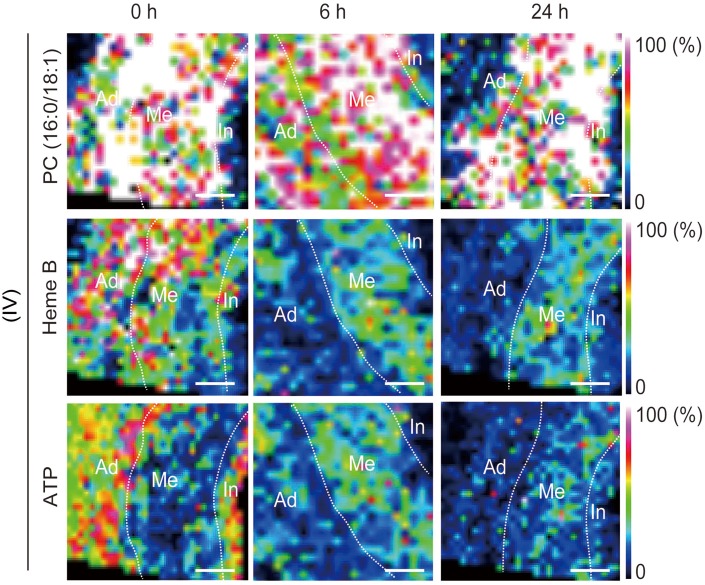
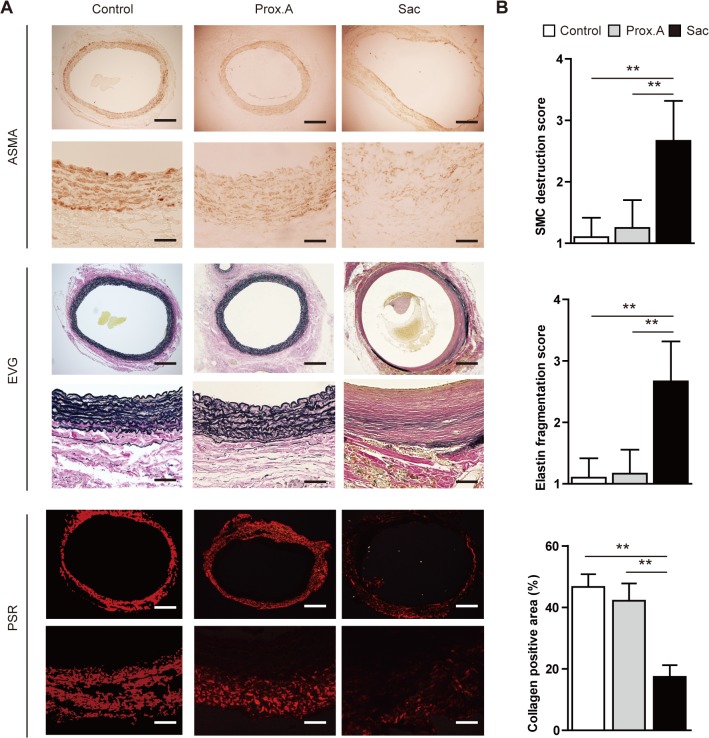
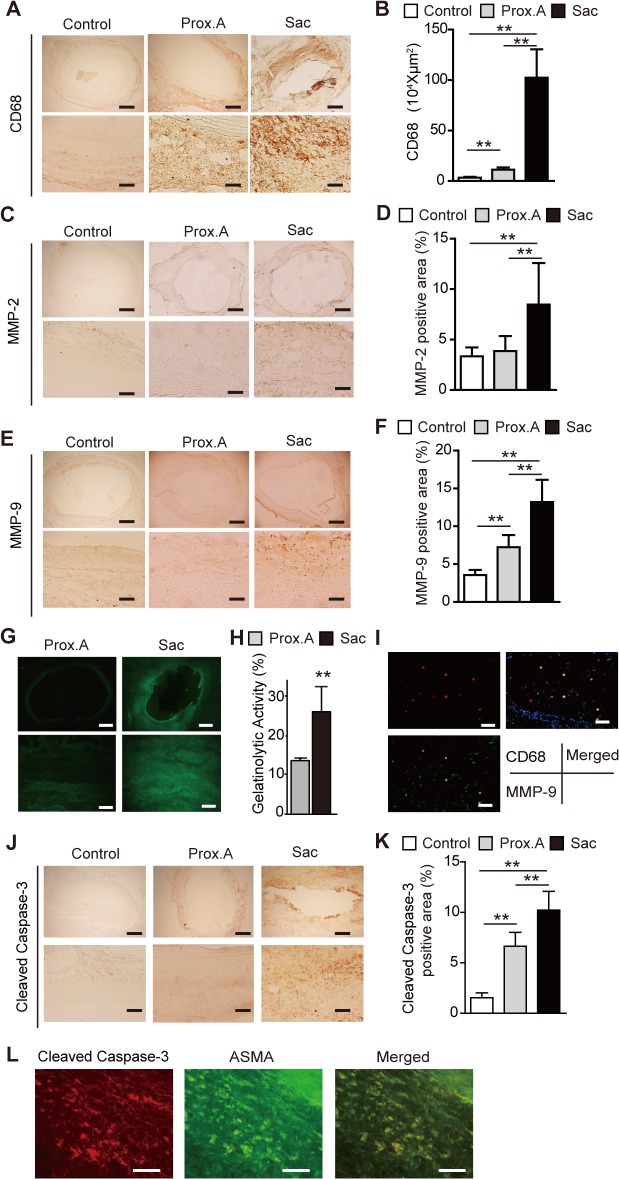
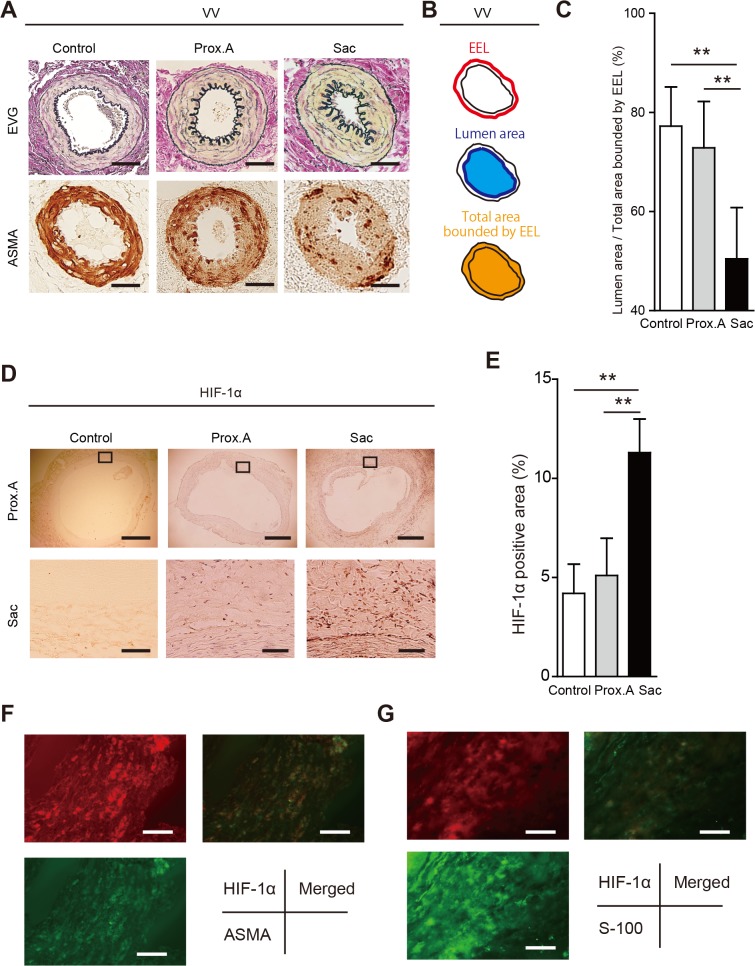
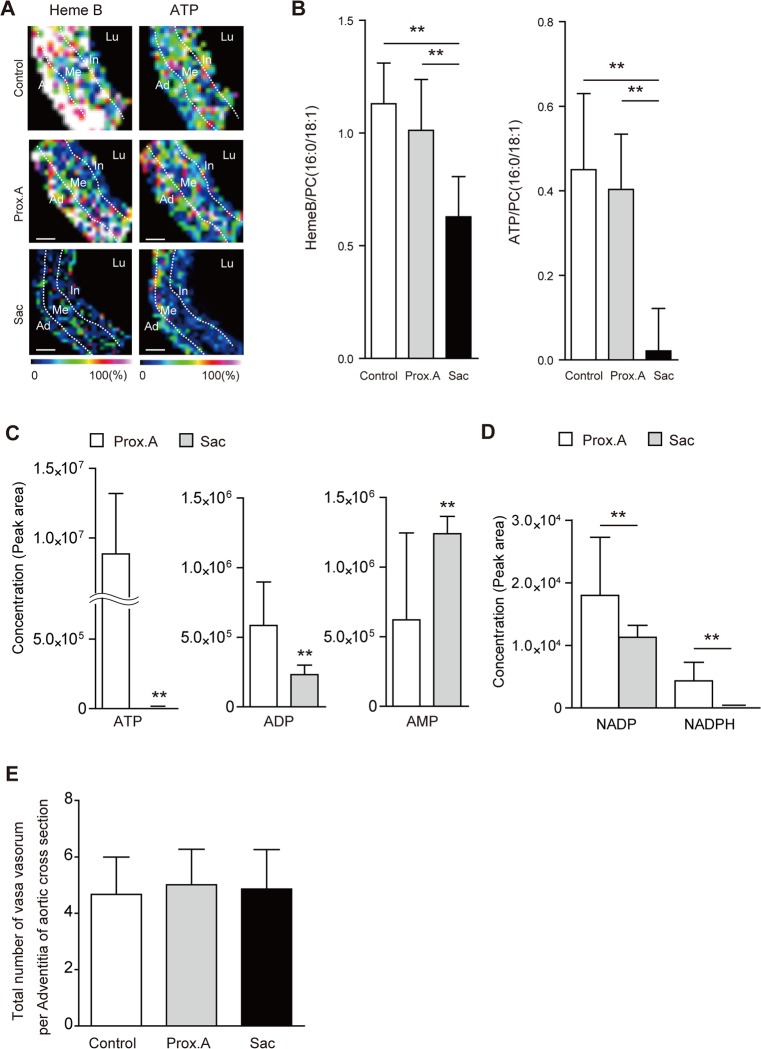
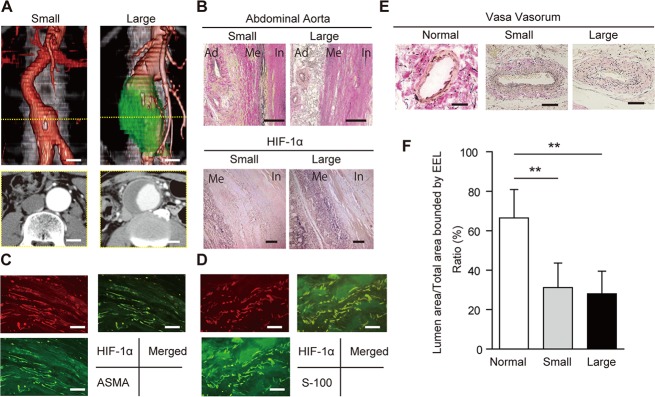
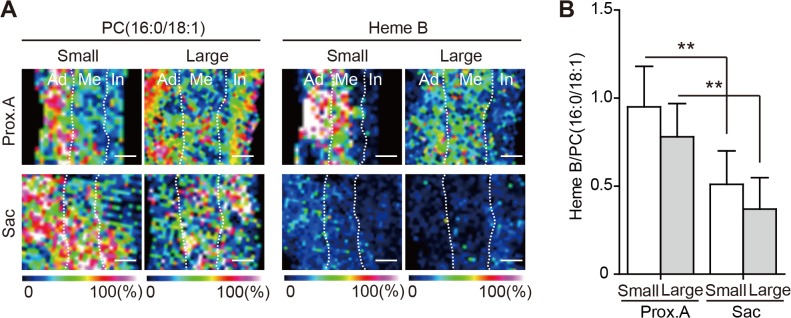
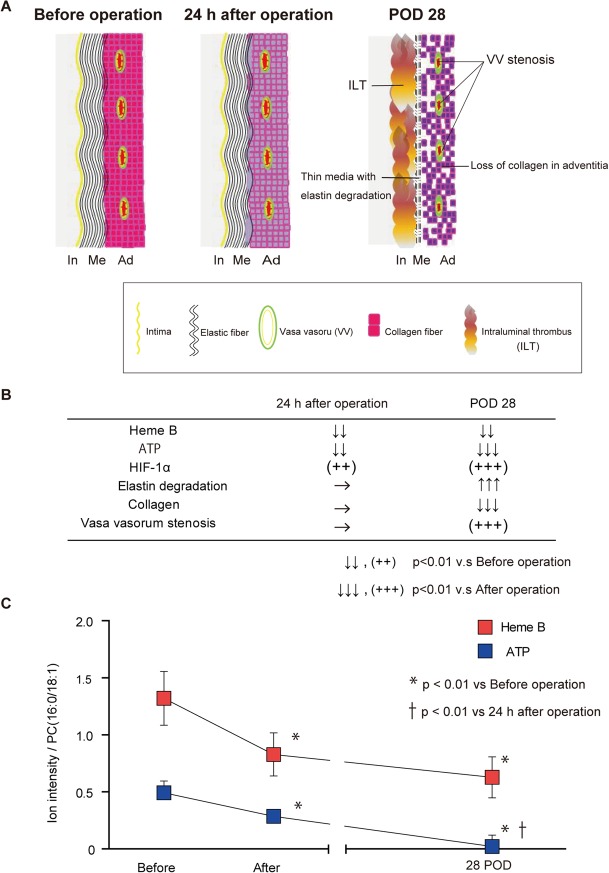
The aortic wall is perfused by the adventitial vasa vasorum (VV). Tissue hypoxia has previously been observed as a manifestation of enlarged abdominal aortic aneurysms (AAAs). We sought to determine whether hypoperfusion of the adventitial VV could develop AAAs. We created a novel animal model of adventitial VV hypoperfusion with a combination of a polyurethane catheter insertion and a suture ligation of the infrarenal abdominal aorta in rats. VV hypoperfusion caused tissue hypoxia and developed infrarenal AAA, which had similar morphological and pathological characteristics to human AAA. In human AAA tissue, the adventitial VV were stenotic in both small AAAs (30-49 mm in diameter) and in large AAAs (> 50 mm in diameter), with the sac tissue in these AAAs being ischemic and hypoxic. These results indicate that hypoperfusion of adventitial VV has critical effects on the development of infrarenal AAA.
Conflict of interest statement
Figures
References
-
- Gandhi RH, Irizarry E, Cantor JO, Keller S, Nackman GB, Halpern VJ, et al. Analysis of elastin cross-linking and the connective tissue matrix of abdominal aortic aneurysms. Surgery. 1994;115:617–620. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
