

Insulin sensitivity of muscle protein metabolism is altered in patients with chronic kidney disease and metabolic acidosis
- PMID: 26308671
- PMCID: PMC4678169
- DOI: 10.1038/ki.2015.247
Insulin sensitivity of muscle protein metabolism is altered in patients with chronic kidney disease and metabolic acidosis
Abstract
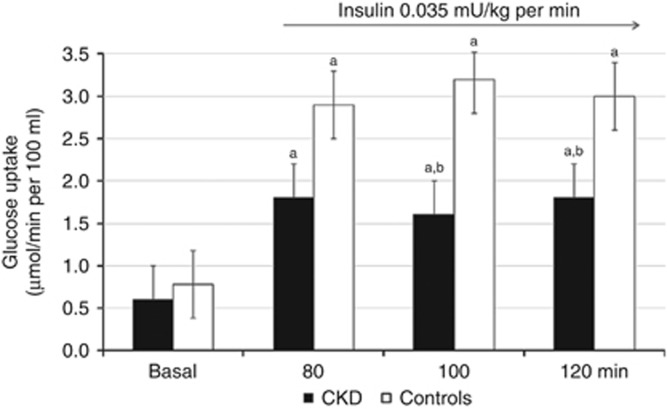
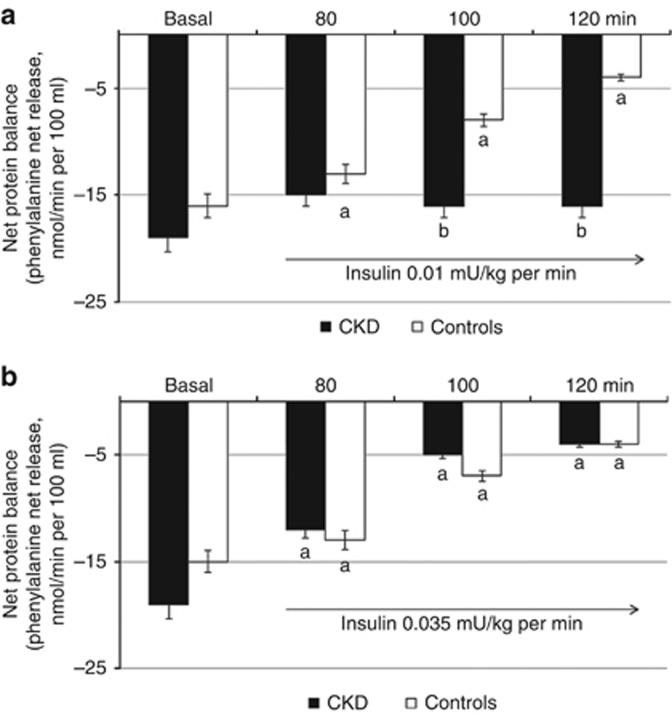
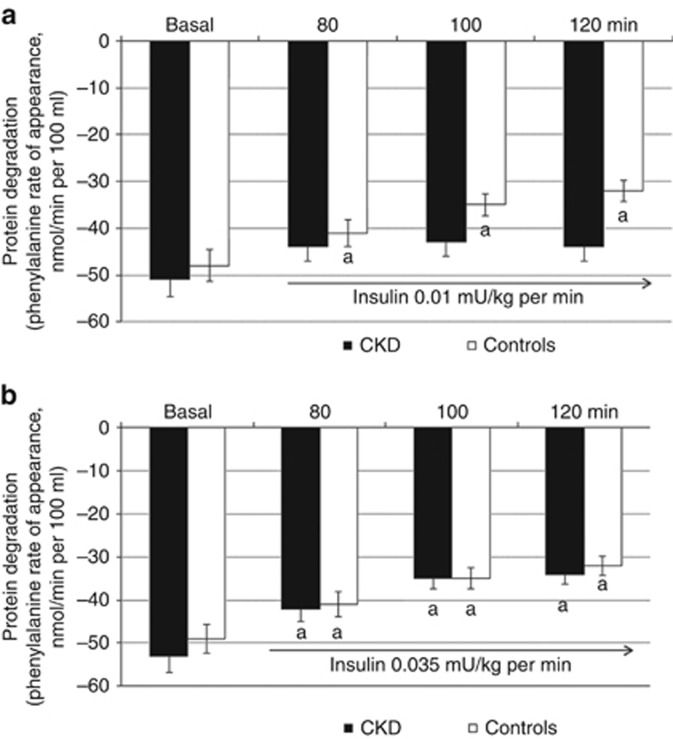
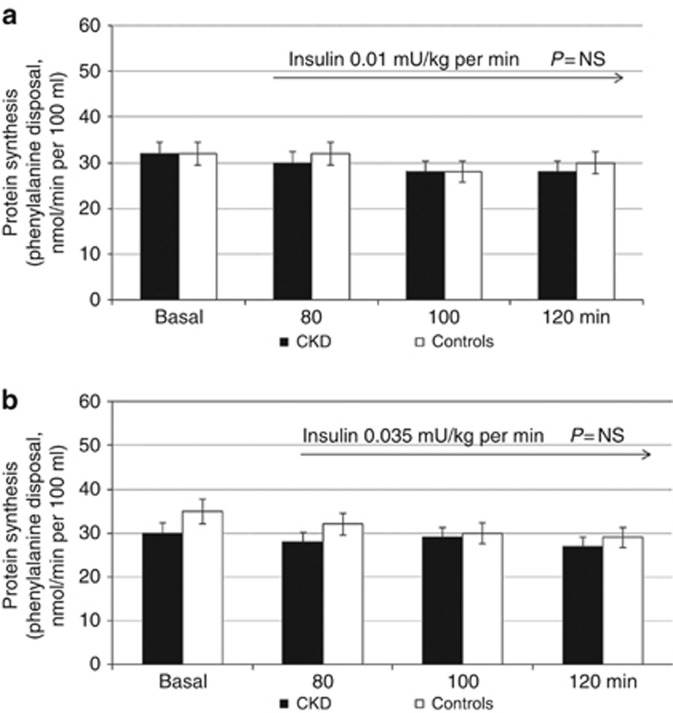
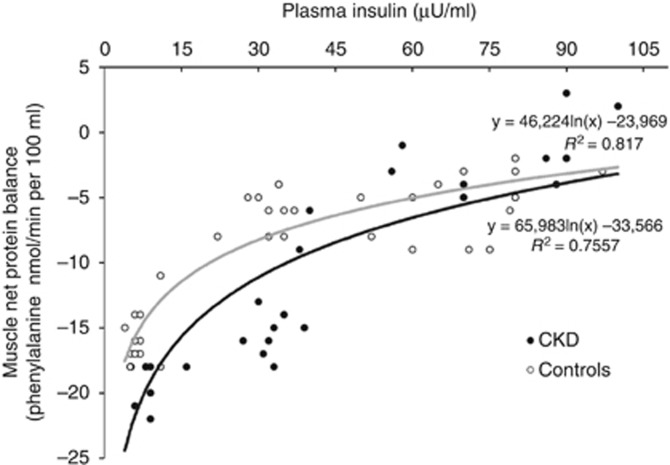
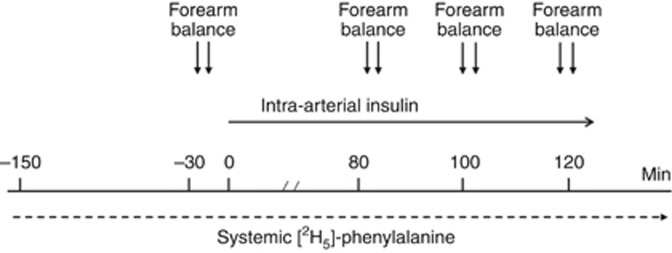
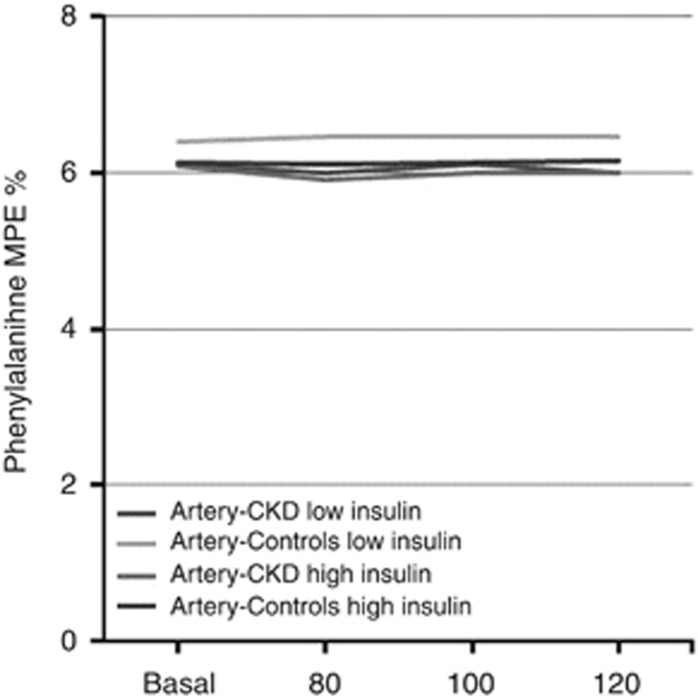
An emergent hypothesis is that a resistance to the anabolic drive by insulin may contribute to loss of strength and muscle mass in patients with chronic kidney disease (CKD). We tested whether insulin resistance extends to protein metabolism using the forearm perfusion method with arterial insulin infusion in 7 patients with CKD and metabolic acidosis (bicarbonate 19 mmol/l) and 7 control individuals. Forearm glucose balance and protein turnover (2H-phenylalanine kinetics) were measured basally and in response to insulin infused at different rates for 2 h to increase local forearm plasma insulin concentration by approximately 20 and 50 μU/ml. In response to insulin, forearm glucose uptake was significantly increased to a lesser extent (-40%) in patients with CKD than controls. In addition, whereas in the controls net muscle protein balance and protein degradation were decreased by both insulin infusion rates, in patients with CKD net protein balance and protein degradation were sensitive to the high (0.035 mU/kg per min) but not the low (0.01 mU/kg per min) insulin infusion. Besides blunting muscle glucose uptake, CKD and acidosis interfere with the normal suppression of protein degradation in response to a moderate rise in plasma insulin. Thus, alteration of protein metabolism by insulin may lead to changes in body tissue composition which may become clinically evident in conditions characterized by low insulinemia.
Figures
References
-
- 1Rigalleau V, Gin H. Carbohydrate metabolism in uraemia. Curr Opin Clin Nutr Metab Care 2005; 8: 463–469. - PubMed
-
- 2Fliser D, Pacini G, Engelleiter R. et al. Insulin resistance and hyperinsulinemia are already present in patients with incipient renal disease. Kidney Int 1998; 53: 1343–1347. - PubMed
-
- 3Kobayashi S, Maesato K, Moriya H et al. Insulin resistance in patients with chronic kidney disease. Am J Kidney Dis 2005; 45: 275–280. - PubMed
-
- 4DeFronzo RA, Smith D, Alvestrand A. Insulin action in uremia. Kidney Int 1983; 24: S102–S114. - PubMed
-
- 5Alvestrand A, Mujagic M, Wajngot A et al. Glucose intolerance in uremic patients: the relative contributions of impaired beta-cell function and insulin resistance. Clin Nephrol 1989; 31: 175–183. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
