

Seizure Outcomes and Predictors of Recurrent Post-Stroke Seizure: A Retrospective Observational Cohort Study
- PMID: 26309124
- PMCID: PMC4550357
- DOI: 10.1371/journal.pone.0136200
Seizure Outcomes and Predictors of Recurrent Post-Stroke Seizure: A Retrospective Observational Cohort Study
Abstract
Background: Seizure is a common complication after stroke (termed "post-stroke seizure," PSS). Although many studies have assessed outcomes and risk factors of PSS, no reliable predictors are currently available to determine PSS recurrence. We compared baseline clinical characteristics and post-stroke treatment regimens between recurrent and non-recurrent PSS patients to identify factors predictive of recurrence.
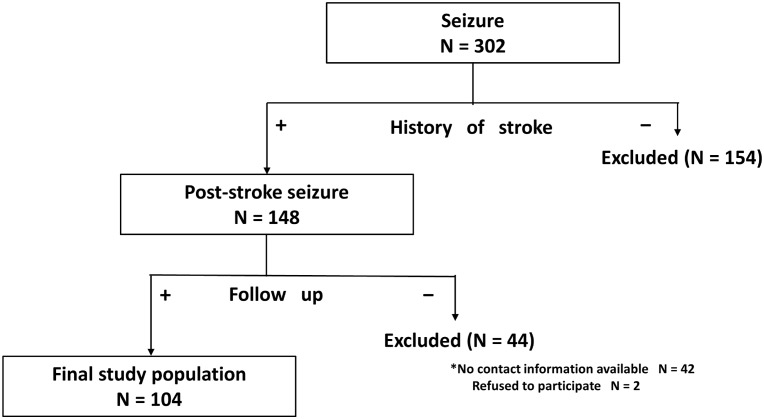
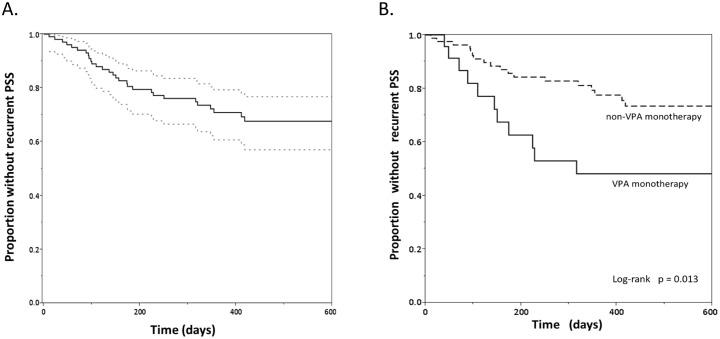
Methods: Consecutive PSS patients admitted to our stroke center between January 2011 and July 2013 were monitored until February 2014 (median 357 days; IQR, 160-552) and retrospectively evaluated for baseline clinical characteristics and PSS recurrence. Cumulative recurrence rates at 90, 180, and 360 days post-stroke were estimated by Kaplan-Meier analysis. Independent predictors of recurrent PSS were identified by Cox proportional-hazards analysis.
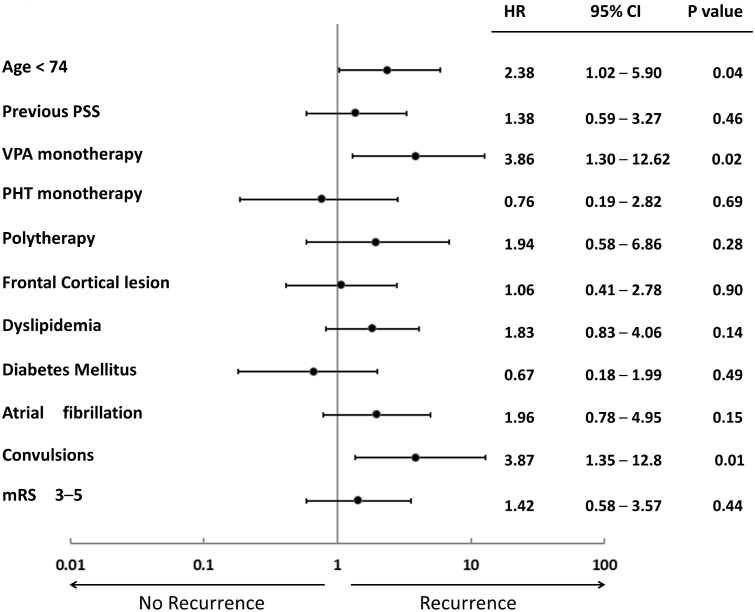
Results: A total of 104 patients (71 men; mean age, 72.1 ± 11.2 years) were analyzed. PSS recurred in 31 patients (30%) during the follow-up. Factors significantly associated with PSS recurrence by log-rank analysis included previous PSS, valproic acid (VPA) monotherapy, polytherapy with antiepileptic drugs (AEDs), frontal cortical lesion, and higher modified Rankin Scale score at discharge (all p < 0.05). Independent predictors of recurrent PSS were age <74 years (HR 2.38, 95% CI 1.02-5.90), VPA monotherapy (HR 3.86, 95% CI 1.30-12.62), and convulsions on admission (HR 3.87, 95% CI 1.35-12.76).
Conclusions: Approximately one-third of PSS patients experienced seizure recurrence within one year. The predictors of recurrent PSS were younger age, presence of convulsions and VPA monotherapy. Our findings should be interpreted cautiously in countries where monotherapy with second-generation AEDs has been approved because this study was conducted while second-generation AEDs had not been officially approved for monotherapy in Japan.
Conflict of interest statement
Figures
Similar articles
-
Risk factors for post-stroke seizure recurrence after the first episode.Seizure. 2017 Nov;52:22-26. doi: 10.1016/j.seizure.2017.09.007. Epub 2017 Sep 14. Seizure. 2017. PMID: 28957721
-
Seizures after intracerebral hemorrhage; risk factor, recurrence, efficacy of antiepileptic drug.J Neurol Sci. 2015 Dec 15;359(1-2):318-22. doi: 10.1016/j.jns.2015.09.358. Epub 2015 Sep 25. J Neurol Sci. 2015. PMID: 26671135
-
Incidence and risk factors of post-stroke seizure among ischemic stroke patients.J Stroke Cerebrovasc Dis. 2024 Dec;33(12):108072. doi: 10.1016/j.jstrokecerebrovasdis.2024.108072. Epub 2024 Oct 12. J Stroke Cerebrovasc Dis. 2024. PMID: 39401576
-
Poststroke seizure: optimising its management.Stroke Vasc Neurol. 2018 Dec 9;4(1):48-56. doi: 10.1136/svn-2018-000175. eCollection 2019 Mar. Stroke Vasc Neurol. 2018. PMID: 31105979 Free PMC article. Review.
-
Post-stroke seizure risk prediction models: a systematic review and meta-analysis.Epileptic Disord. 2022 Apr 1;24(2):302-314. doi: 10.1684/epd.2021.1391. Epileptic Disord. 2022. PMID: 34874273
Cited by
-
Risk Factors Associated with Epilepsy Related to Cerebrovascular Disease: A Systematic Review and Meta-Analysis.Neuropsychiatr Dis Treat. 2023 Dec 27;19:2841-2856. doi: 10.2147/NDT.S439995. eCollection 2023. Neuropsychiatr Dis Treat. 2023. PMID: 38161512 Free PMC article. Review.
-
Interictal epileptiform discharges as a predictive biomarker for recurrence of poststroke epilepsy.Brain Commun. 2022 Nov 26;4(6):fcac312. doi: 10.1093/braincomms/fcac312. eCollection 2022. Brain Commun. 2022. PMID: 36523270 Free PMC article.
-
Short duration of focal onset awareness and impaired awareness seizure are characteristic features of epilepsy in elderly patients.Neuropsychiatr Dis Treat. 2018 Oct 30;14:2879-2887. doi: 10.2147/NDT.S179720. eCollection 2018. Neuropsychiatr Dis Treat. 2018. PMID: 30464472 Free PMC article.
-
Risk Factors for Epilepsy After Thrombolysis for Ischemic Stroke: A Cohort Study.Front Neurol. 2020 Jan 23;10:1256. doi: 10.3389/fneur.2019.01256. eCollection 2019. Front Neurol. 2020. PMID: 32038448 Free PMC article.
-
Characteristics of the patients who admitted to the emergency department with seizures and the factors affecting the frequency of admission.Neurosciences (Riyadh). 2021 Apr;26(2):163-170. doi: 10.17712/nsj.2021.2.20200092. Neurosciences (Riyadh). 2021. PMID: 33814369 Free PMC article.
References
-
- Bladin CF, Alexandrov AV, Bellavance A, Bornstein N, Chambers B, Cote R, et al. Seizures after stroke: a prospective multicenter study. Arch Neurol. 2000;57(11):1617–22. Epub 2000/11/14. noc90169 [pii]. . - PubMed
-
- So EL, Annegers JF, Hauser WA, O'Brien PC, Whisnant JP. Population-based study of seizure disorders after cerebral infarction. Neurology. 1996;46(2):350–5. Epub 1996/02/01. . - PubMed
-
- Kraus JA, Berlit P. Cerebral embolism and epileptic seizures—the role of the embolic source. Acta Neurol Scand. 1998;97(3):154–9. Epub 1998/04/08. . - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
