

OCT angiography by absolute intensity difference applied to normal and diseased human retinas
- PMID: 26309740
- PMCID: PMC4541504
- DOI: 10.1364/BOE.6.002738
OCT angiography by absolute intensity difference applied to normal and diseased human retinas
Abstract
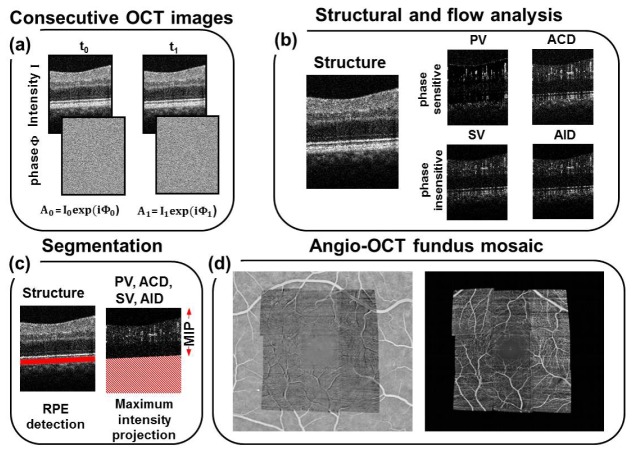
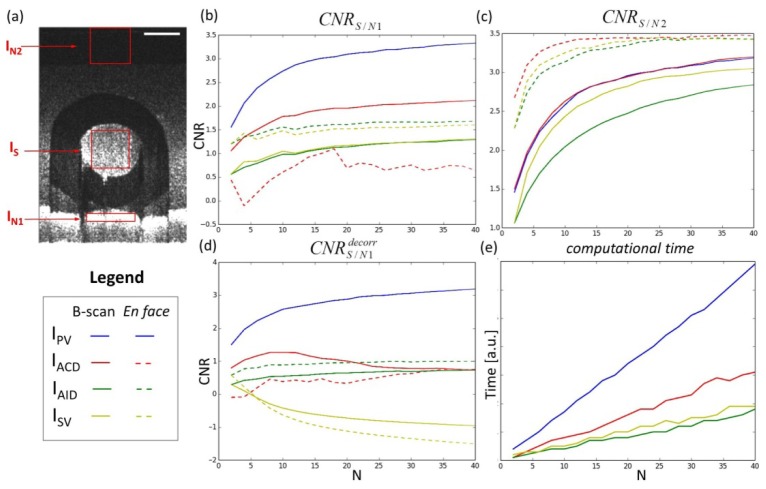
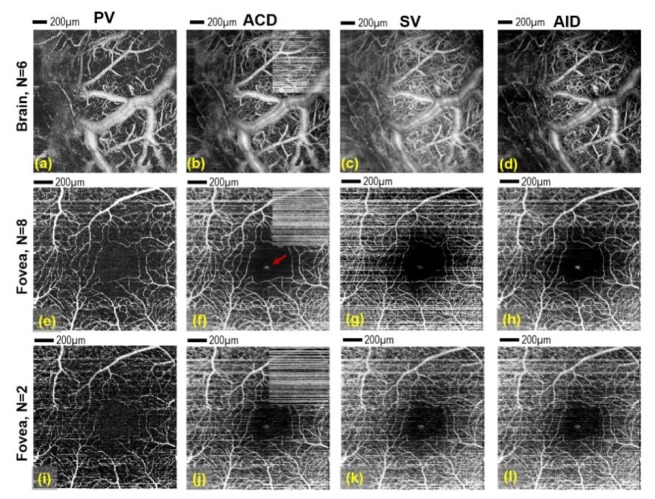
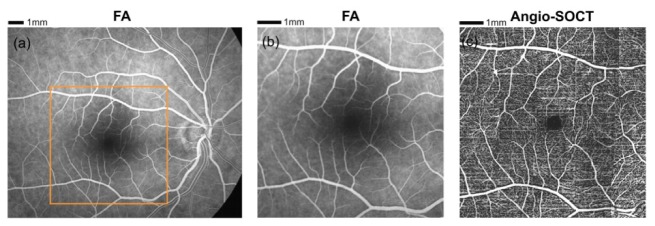
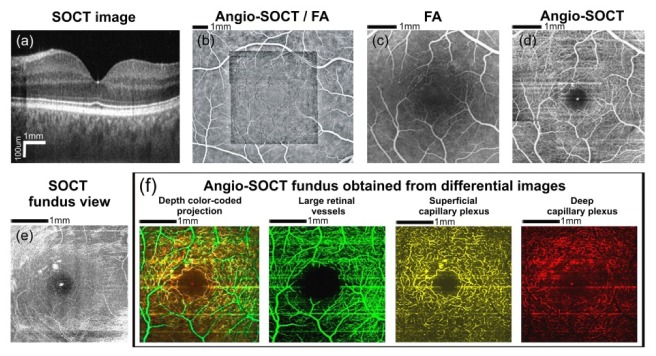
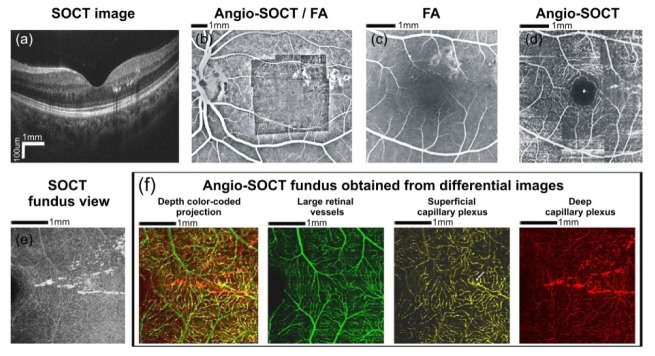
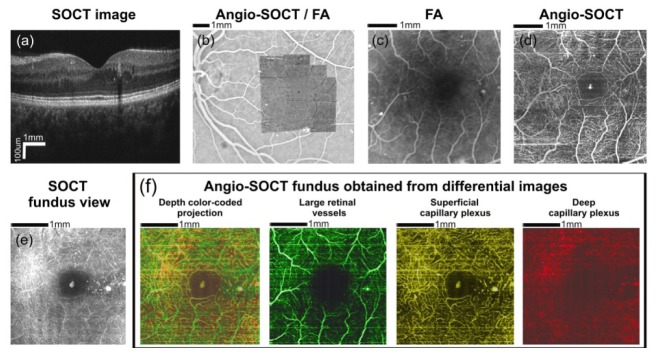
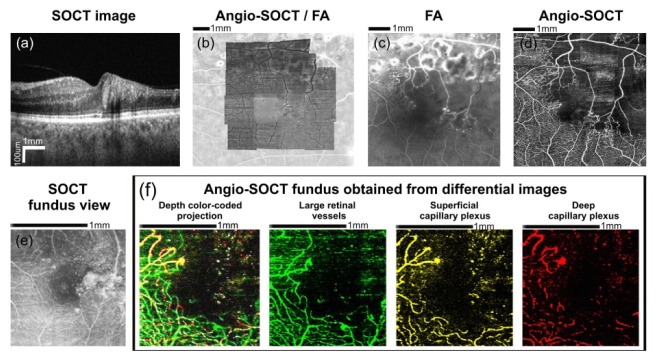
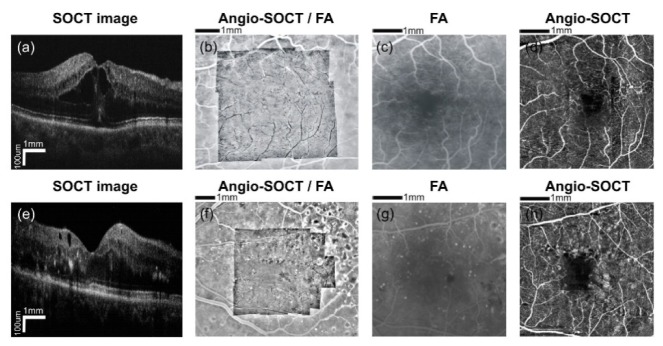
We compare four optical coherence tomography techniques for noninvasive visualization of microcapillary network in the human retina and murine cortex. We perform phantom studies to investigate contrast-to-noise ratio for angiographic images obtained with each of the algorithm. We show that the computationally simplest absolute intensity difference angiographic OCT algorithm that bases only on two cross-sectional intensity images may be successfully used in clinical study of healthy eyes and eyes with diabetic maculopathy and branch retinal vein occlusion.
Keywords: (110.4500) Optical coherence tomography; (170.3880) Medical and biological imaging; (170.4470) Ophthalmology; (280.2490) Flow diagnostics.
Figures
References
-
- Vakoc B. J., Lanning R. M., Tyrrell J. A., Padera T. P., Bartlett L. A., Stylianopoulos T., Munn L. L., Tearney G. J., Fukumura D., Jain R. K., Bouma B. E., “Three-dimensional microscopy of the tumor microenvironment in vivo using optical frequency domain imaging,” Nat. Med. 15(10), 1219–1223 (2009). 10.1038/nm.1971 - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources