

A systematic review and meta-analysis of randomized controlled trials of endovascular thrombectomy compared with best medical treatment for acute ischemic stroke
- PMID: 26310289
- PMCID: PMC5102634
- DOI: 10.1111/ijs.12618
A systematic review and meta-analysis of randomized controlled trials of endovascular thrombectomy compared with best medical treatment for acute ischemic stroke
Erratum in
-
Corrigendum to a systematic review and meta-analysis of randomized controlled trials of endovascular thrombectomy compared to best medical treatment for acute ischemic stroke.Int J Stroke. 2017 Jan;12(1):NP7. doi: 10.1177/1747493016675982. Epub 2016 Nov 19. Int J Stroke. 2017. PMID: 27856819 Free PMC article. No abstract available.
Abstract
Background: Acute ischemic strokes involving occlusion of large vessels usually recanalize poorly following treatment with intravenous thrombolysis. Recent studies have shown higher recanalization and higher good outcome rates with endovascular therapy compared with best medical management alone. A systematic review and meta-analysis investigating the benefits of all randomized controlled trials of endovascular thrombectomy where at least 25% of patients were treated with a thrombectomy device for the treatment of acute ischemic stroke compared with best medical treatment have yet to be performed.
Aim: To perform a systematic review and a meta-analysis evaluating the effectiveness of endovascular thrombectomy compared with best medical care for treatment of acute ischemic stroke.
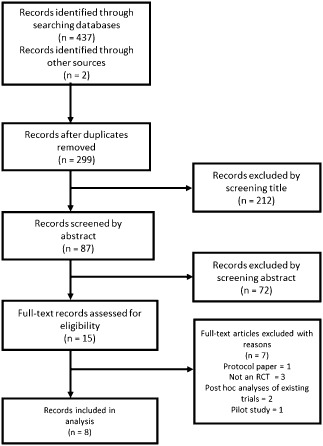
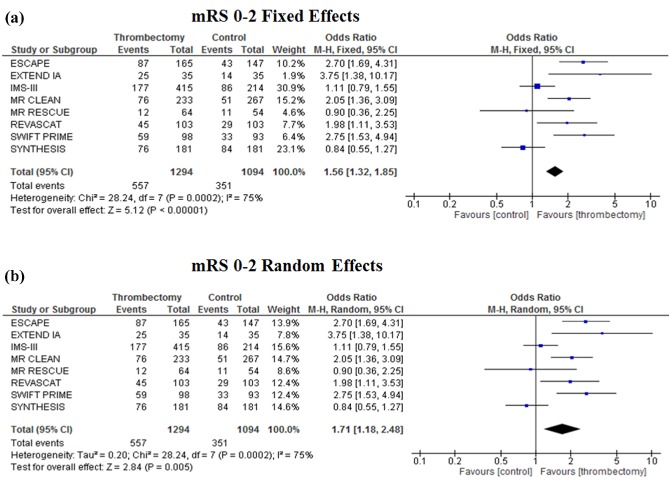
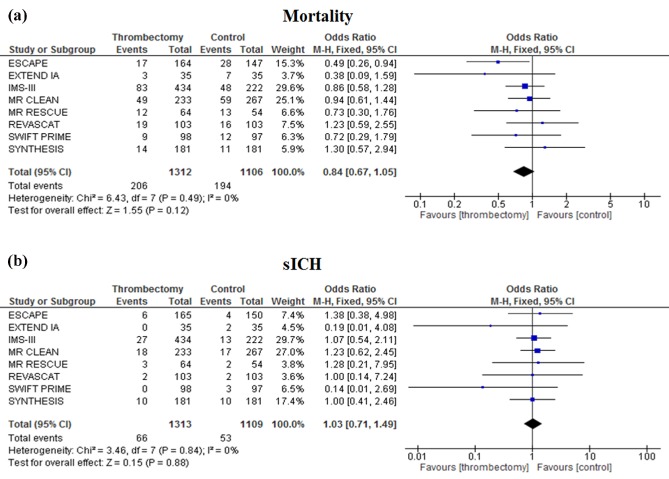
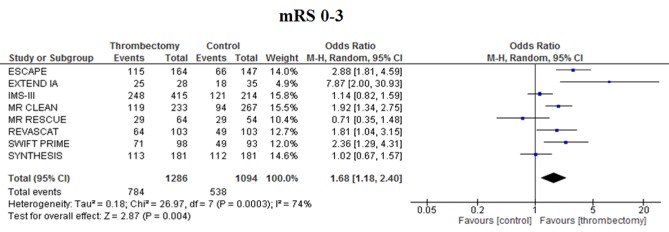
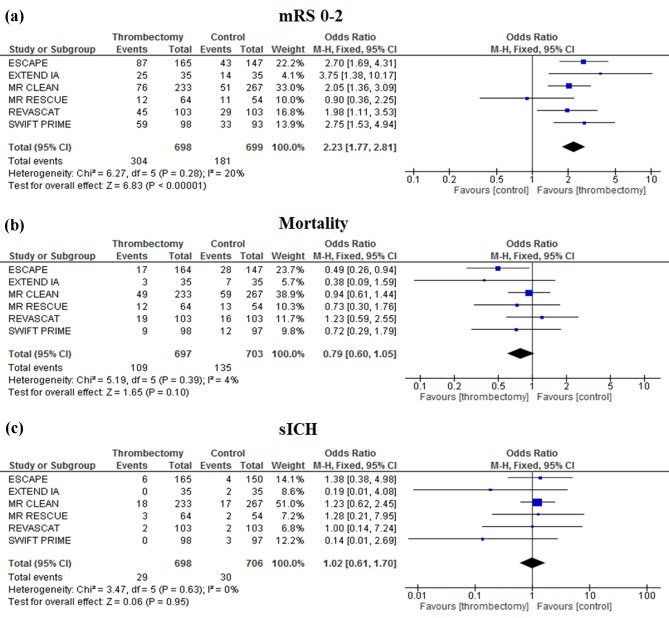
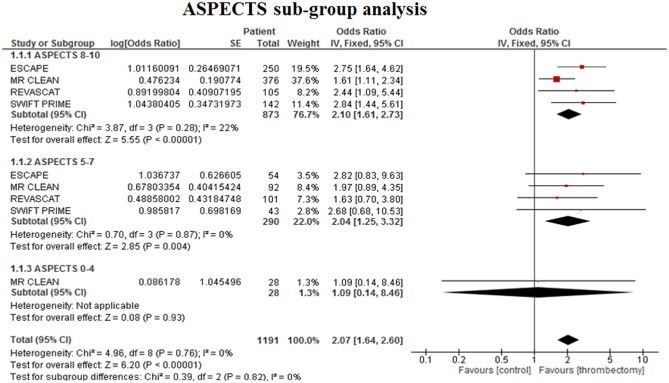
Summary of review: Our search identified 437 publications, from which eight studies (totaling 2423 patients) matched the inclusion criteria. Overall, endovascular thrombectomy was associated with improved functional outcomes (modified Rankin Scale 0-2) [odds ratio 1·56 (1·32-1·85), P < 0·00001]. There was a tendency toward decreased mortality [odds ratio 0·84 (0·67-1·05), P = 0·12], and symptomatic intracerebral hemorrhage was not increased [odds ratio 1·03 (0·71-1·49), P = 0·88] compared with best medical management alone. The odds ratio for a favorable functional outcome increased to 2·23 (1·77-2·81, P < 0·00001) when newer generation thrombectomy devices were used in greater than 50% of the cases in each trial.
Conclusions: There is clear evidence for improvement in functional independence with endovascular thrombectomy compared with standard medical care, suggesting that endovascular thrombectomy should be considered the standard effective treatment alongside thombolysis in eligible patients.
Keywords: endovascular therapy/treatment; intravenous thrombolysis; ischemic stroke; meta-analysis; systematic review; thrombectomy.
© 2015 The Authors. International Journal of Stroke published by John Wiley & Sons Ltd on behalf of World Stroke Organization.
Figures
References
-
- Lima FO, Furie KL, Silva GS et al Prognosis of untreated strokes due to anterior circulation proximal intracranial arterial occlusions detected by use of computed tomography angiography. JAMA Neurol 2014; 71:151–157. - PubMed
-
- Rha JH, Saver JL. The impact of recanalization on ischemic stroke outcome: a meta‐analysis. Stroke 2007; 38:967–973. - PubMed
-
- Mokin M, Kass‐Hout T, Kass‐Hout O et al Intravenous thrombolysis and endovascular therapy for acute ischemic stroke with internal carotid artery occlusion: a systematic review of clinical outcomes. Stroke 2012; 43:2362–2368. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
