

Laser capture microdissection as a tool to evaluate human papillomavirus genotyping and methylation as biomarkers of persistence and progression of anal lesions
- PMID: 26310402
- PMCID: PMC4554896
- DOI: 10.1136/bmjopen-2015-008439
Laser capture microdissection as a tool to evaluate human papillomavirus genotyping and methylation as biomarkers of persistence and progression of anal lesions
Abstract
Introduction: Anal squamous cell carcinoma is preceded by persistent infection with high-risk human papillomavirus (HPV) and the cancer precursor, high-grade squamous intraepithelial lesion (HSIL). Detection of specific HPV genotypes and HPV-related biomarkers may be an option for primary anal screening. However, more data on the natural history of HPV-related anal lesions are required. The outcomes from this study will enhance our understanding of the clinical and biological behaviour of HPV-related anal lesions and inform the development of future HPV genotype and/or biomarker screening tests.
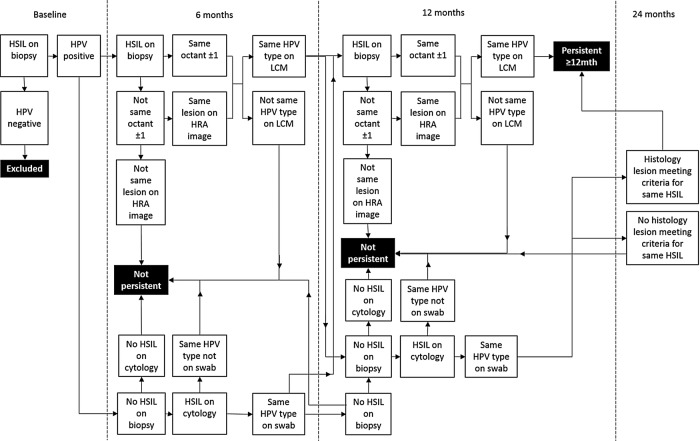
Methods and analysis: HIV-negative and HIV-positive men who have sex with men, aged 35 years and over, recruited from community-based settings in Sydney, Australia, attend 6 clinic visits over 3 years. At the first 5 visits, participants undergo a digital anorectal examination, an anal swab for HPV genotyping and anal cytology, and high-resolution anoscopy with directed biopsy of any visible abnormalities that are suggestive of any abnormality suspicious of SIL. Tissue sections from participants diagnosed with histologically confirmed HSIL at the baseline clinic visit will undergo laser capture microdissection, HPV detection and genotyping, and quantitation of CpG methylation in baseline and follow-up biopsies. Histological and cytological findings in combination with HPV genotyping data will be used to identify persistent HSIL. HSIL will be stratified as non-persistent and persistent based on their status at 12 months. The performance of HPV genotype and methylation status in predicting disease persistence at 12 months will be assessed, along with associations with HIV status and other covariates such as age.
Ethics and dissemination: The St Vincent's Hospital Ethics Committee granted ethics approval for the study. Written informed consent is obtained from all individuals before any study-specific procedures are performed. Findings from this study will be disseminated to participants and the community through study newsletters, and through peer-reviewed publications and international conferences.
Keywords: Anal cancer; Biomarkers; HSIL/HGAIN; Human papillomavirus; Laser capture microdissection; Precancerous conditions.
Published by the BMJ Publishing Group Limited. For permission to use (where not already granted under a licence) please go to http://group.bmj.com/group/rights-licensing/permissions.
Figures




References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical