

Implant Design Variations in Reverse Total Shoulder Arthroplasty Influence the Required Deltoid Force and Resultant Joint Load
- PMID: 26310680
- PMCID: PMC4586233
- DOI: 10.1007/s11999-015-4526-0
Implant Design Variations in Reverse Total Shoulder Arthroplasty Influence the Required Deltoid Force and Resultant Joint Load
Abstract
Background: Reverse total shoulder arthroplasty (RTSA) is widely used; however, the effects of RTSA geometric parameters on joint and muscle loading, which strongly influence implant survivorship and long-term function, are not well understood. By investigating these parameters, it should be possible to objectively optimize RTSA design and implantation technique.
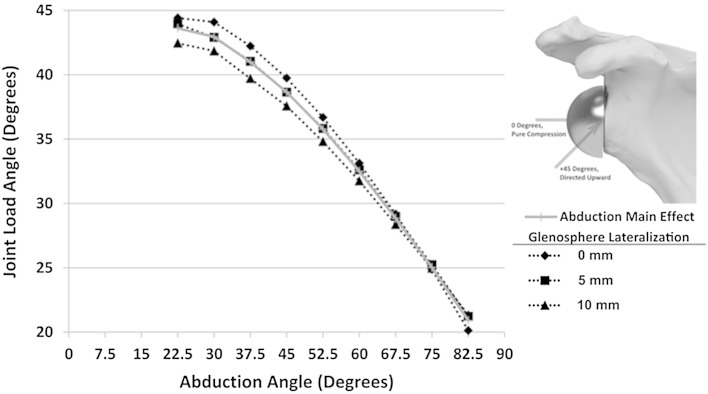
Questions/purposes: The purposes of this study were to evaluate the effect of RTSA implant design parameters on (1) the deltoid muscle forces required to produce abduction, and (2) the magnitude of joint load and (3) the loading angle throughout this motion. We also sought to determine how these parameters interacted.
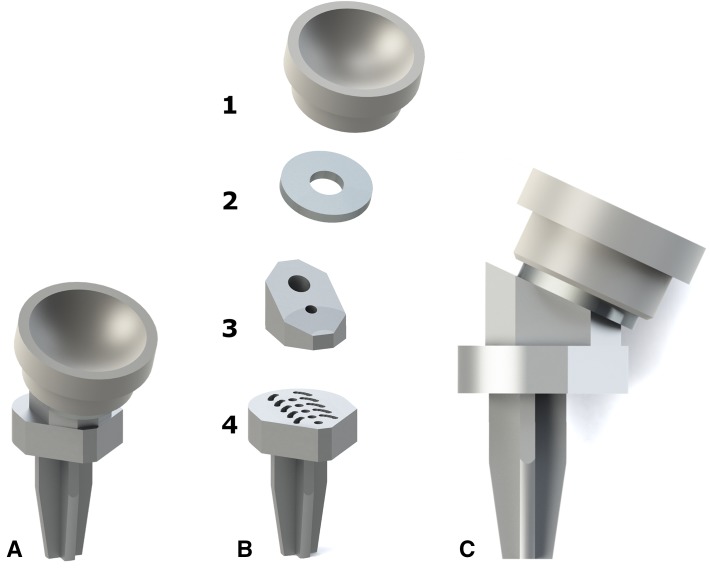
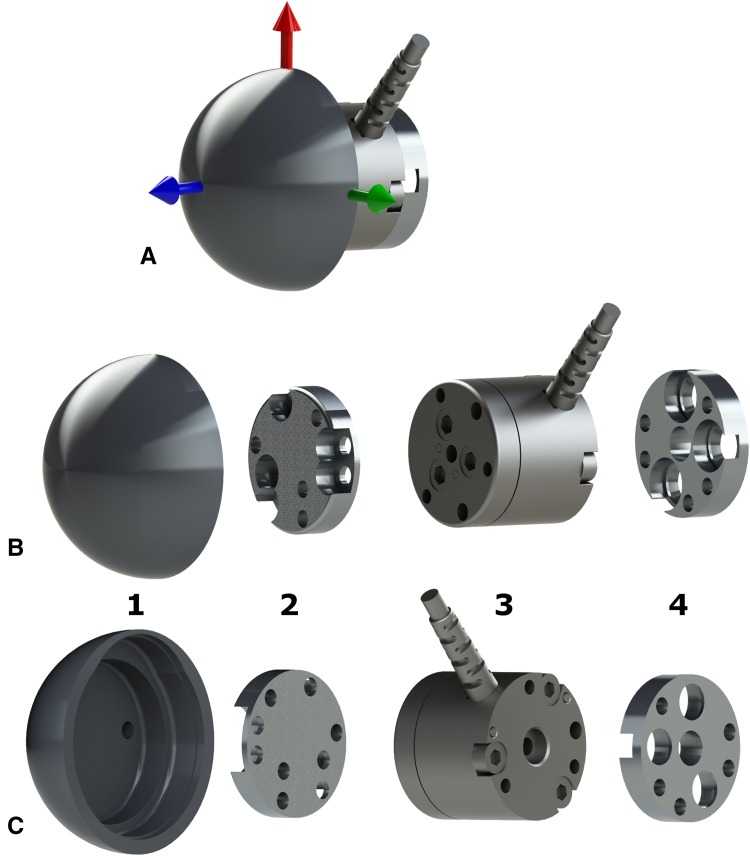
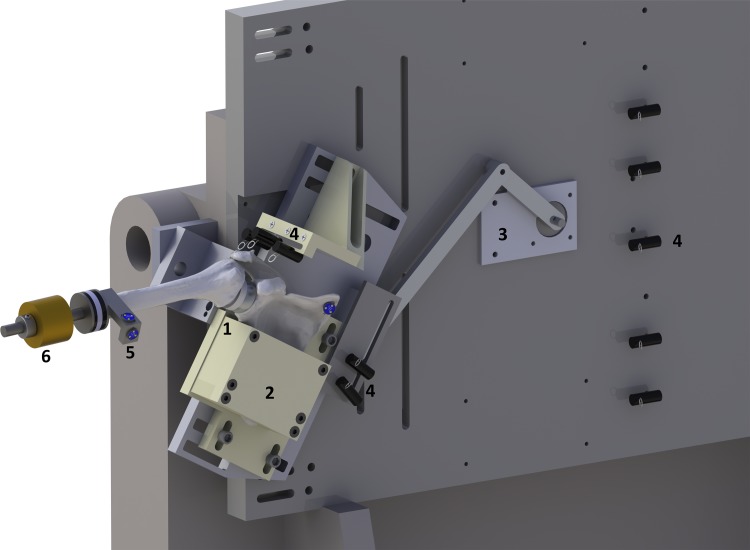
Methods: Seven cadaveric shoulders were tested using a muscle load-driven in vitro simulator to achieve repeatable motions. The effects of three implant parameters-humeral lateralization (0, 5, 10 mm), polyethylene thickness (3, 6, 9 mm), and glenosphere lateralization (0, 5, 10 mm)-were assessed for the three outcomes: deltoid muscle force required to produce abduction, magnitude of joint load, and joint loading angle throughout abduction.
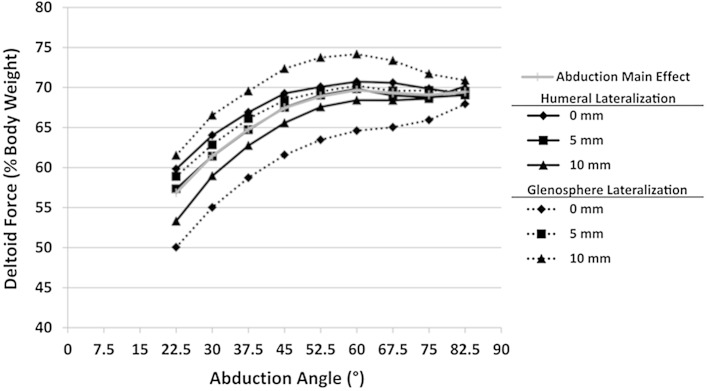
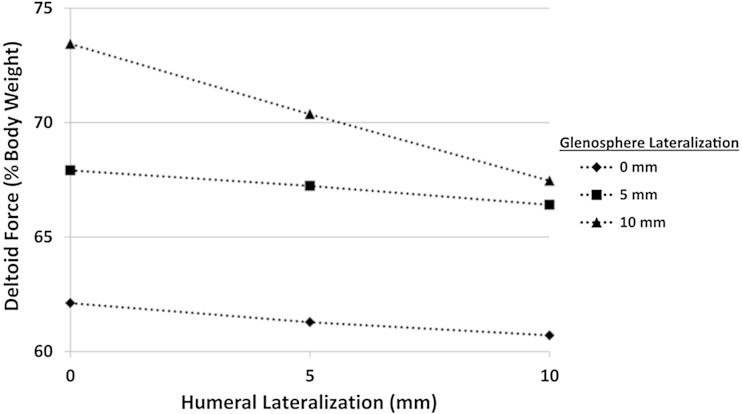
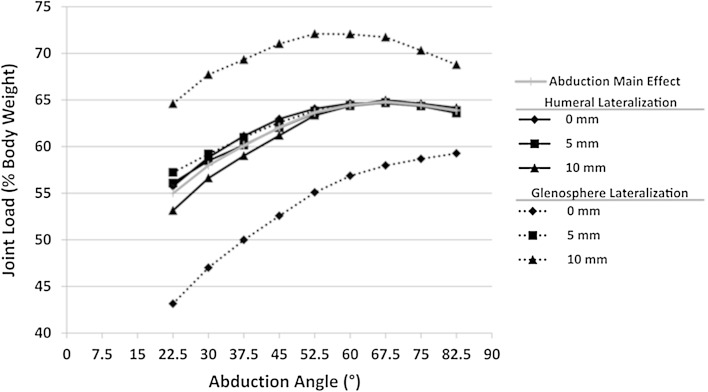
Results: Increasing humeral lateralization decreased deltoid forces required for active abduction (0 mm: 68% ± 8% [95% CI, 60%-76% body weight (BW)]; 10 mm: 65% ± 8% [95% CI, 58%-72 % BW]; p = 0.022). Increasing glenosphere lateralization increased deltoid force (0 mm: 61% ± 8% [95% CI, 55%-68% BW]; 10 mm: 70% ± 11% [95% CI, 60%-81% BW]; p = 0.007) and joint loads (0 mm: 53% ± 8% [95% CI, 46%-61% BW]; 10 mm: 70% ± 10% [95% CI, 61%-79% BW]; p < 0.001). Increasing polyethylene cup thickness increased deltoid force (3 mm: 65% ± 8% [95% CI, 56%-73% BW]; 9 mm: 68% ± 8% [95% CI, 61%-75% BW]; p = 0.03) and joint load (3 mm: 60% ± 8% [95% CI, 53%-67% BW]; 9 mm: 64% ± 10% [95% CI, 56%-72% BW]; p = 0.034).
Conclusions: Humeral lateralization was the only parameter that improved joint and muscle loading, whereas glenosphere lateralization resulted in increased loads. Humeral lateralization may be a useful implant parameter in countering some of the negative effects of glenosphere lateralization, but this should not be considered the sole solution for the negative effects of glenosphere lateralization. Overstuffing the articulation with progressively thicker humeral polyethylene inserts produced some adverse effects on deltoid muscle and joint loading.
Clinical relevance: This systematic evaluation has determined that glenosphere lateralization produces marked negative effects on loading outcomes; however, the importance of avoiding scapular notching may outweigh these effects. Humeral lateralization's ability to decrease the effects of glenosphere lateralization was promising but further investigations are required to determine the effects of combined lateralization on functional outcomes including range of motion.
Figures
Comment in
-
CORR Insights(®): implant design variations in reverse total shoulder arthroplasty influence the required deltoid force and resultant joint load.Clin Orthop Relat Res. 2015 Dec;473(12):3940-2. doi: 10.1007/s11999-015-4551-z. Epub 2015 Sep 22. Clin Orthop Relat Res. 2015. PMID: 26394637 Free PMC article. No abstract available.
References
-
- Archard JF. Contact and rubbing of flat surfaces. J Appl Phys. 1953;24:981–988. doi: 10.1063/1.1721448. - DOI
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
