

The associations between daily spring pollen counts, over-the-counter allergy medication sales, and asthma syndrome emergency department visits in New York City, 2002-2012
- PMID: 26310854
- PMCID: PMC4549916
- DOI: 10.1186/s12940-015-0057-0
The associations between daily spring pollen counts, over-the-counter allergy medication sales, and asthma syndrome emergency department visits in New York City, 2002-2012
Abstract
Background: Many types of tree pollen trigger seasonal allergic illness, but their population-level impacts on allergy and asthma morbidity are not well established, likely due to the paucity of long records of daily pollen data that allow analysis of multi-day effects. Our objective in this study was therefore to determine the impacts of individual spring tree pollen types on over-the-counter allergy medication sales and asthma emergency department (ED) visits.
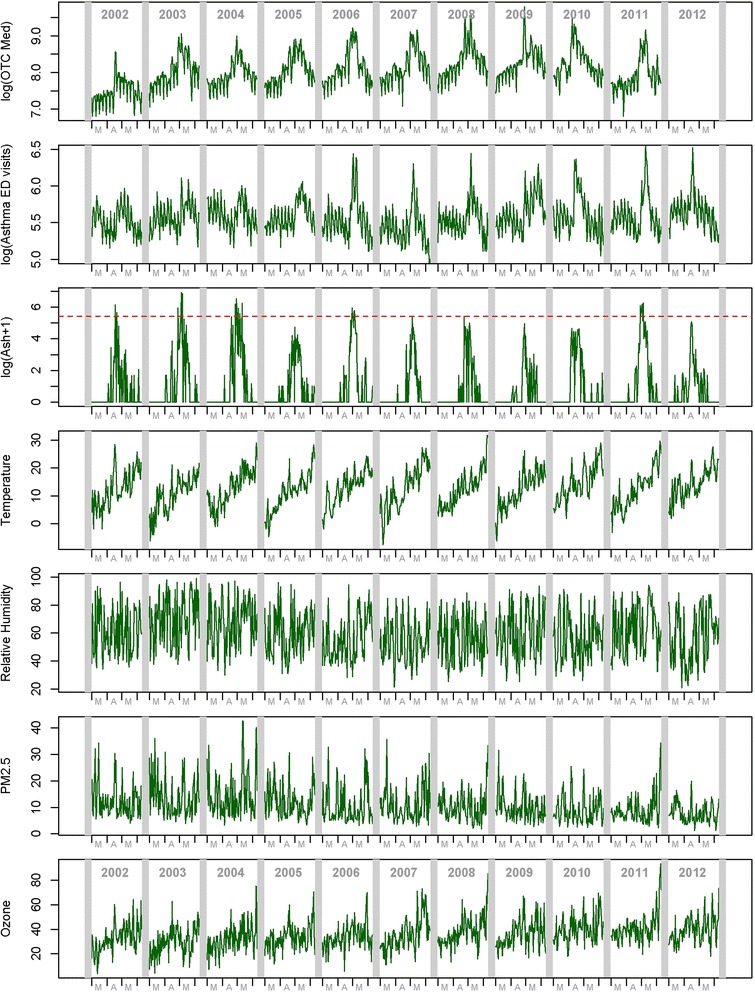
Methods: Nine clinically-relevant spring tree pollen genera (elm, poplar, maple, birch, beech, ash, sycamore/London planetree, oak, and hickory) measured in Armonk, NY, were analyzed for their associations with over-the-counter allergy medication sales and daily asthma syndrome ED visits from patients' chief complaints or diagnosis codes in New York City during March 1st through June 10th, 2002-2012. Multi-day impacts of pollen on the outcomes (0-3 days and 0-7 days for the medication sales and ED visits, respectively) were estimated using a distributed lag Poisson time-series model adjusting for temporal trends, day-of-week, weather, and air pollution. For asthma syndrome ED visits, age groups were also analyzed. Year-to-year variation in the average peak dates and the 10th-to-90th percentile duration between pollen and the outcomes were also examined with Spearman's rank correlation.
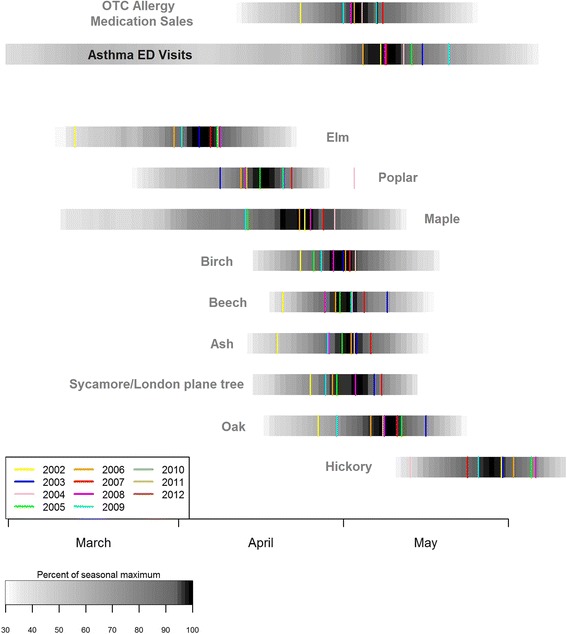
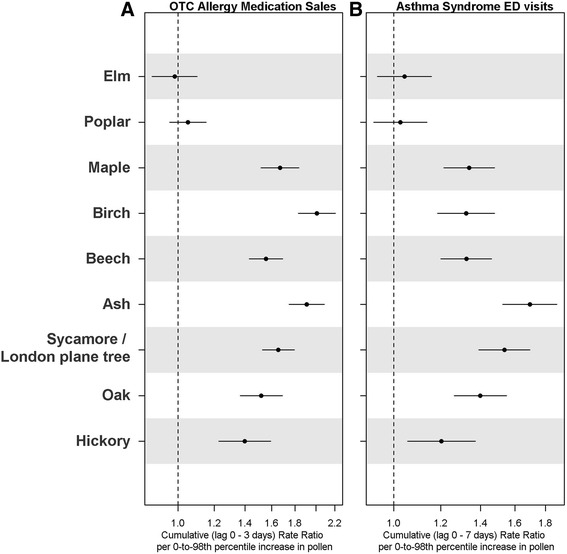
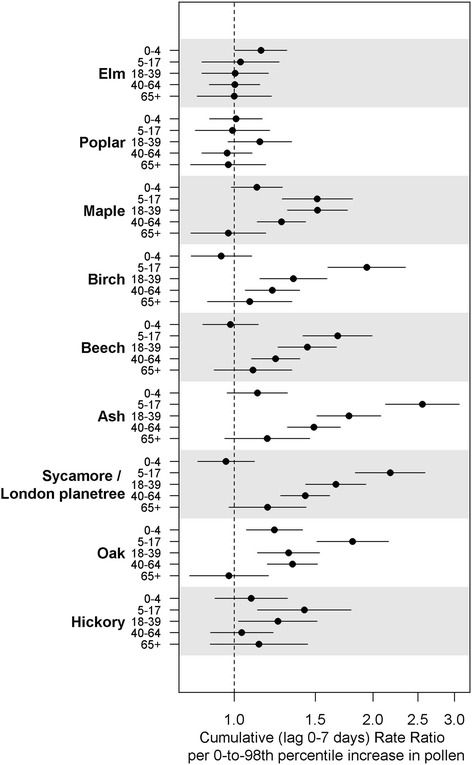
Results: Mid-spring pollen types (maple, birch, beech, ash, oak, and sycamore/London planetree) showed the strongest significant associations with both outcomes, with cumulative rate ratios up to 2.0 per 0-to-98th percentile pollen increase (e.g., 1.9 [95% CI: 1.7, 2.1] and 1.7 [95% CI: 1.5, 1.9] for the medication sales and ED visits, respectively, for ash). Lagged associations were longer for asthma syndrome ED visits than for the medication sales. Associations were strongest in children (ages 5-17; e.g., a cumulative rate ratio of 2.6 [95% CI: 2.1, 3.1] per 0-to-98th percentile increase in ash). The average peak dates and durations of some of these mid-spring pollen types were also associated with those of the outcomes.
Conclusions: Tree pollen peaking in mid-spring exhibit substantive impacts on allergy, and asthma exacerbations, particularly in children. Given the narrow time window of these pollen peak occurrences, public health and clinical approaches to anticipate and reduce allergy/asthma exacerbation should be developed.
Figures
References
-
- Lin RY, Clauss AE, Bennett ES. Hypersensitivity to common tree pollens in New York City patients. Allergy Asthma Proc. 2002;23(4):253–258. - PubMed
-
- Fuhrman C, Sarter H, Thibaudon M, Delmas MC, Zeghnoun A, Lecadet J, Caillaud D. Short-term effect of pollen exposure on antiallergic drug consumption. Allergy Asthma Proc. 2007;99(3):225–231. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- K23ES024127/ES/NIEHS NIH HHS/United States
- T32ES007322/ES/NIEHS NIH HHS/United States
- P30 ES000260/ES/NIEHS NIH HHS/United States
- T32HD049311/HD/NICHD NIH HHS/United States
- P30 ES023515/ES/NIEHS NIH HHS/United States
- P30-ES00260/ES/NIEHS NIH HHS/United States
- T32 HD049311/HD/NICHD NIH HHS/United States
- T32 ES007322/ES/NIEHS NIH HHS/United States
- K23 ES024127/ES/NIEHS NIH HHS/United States
- 200-2009-31909-003/PHS HHS/United States
- T32 ES023770/ES/NIEHS NIH HHS/United States
- P30 ES009089/ES/NIEHS NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
