Pulmonary Tumor Thrombotic Microangiopathy: Clinical, Radiologic, and Histologic Correlation
- PMID: 26312142
- PMCID: PMC4541166
- DOI: 10.4103/2156-7514.161978
Pulmonary Tumor Thrombotic Microangiopathy: Clinical, Radiologic, and Histologic Correlation
Abstract
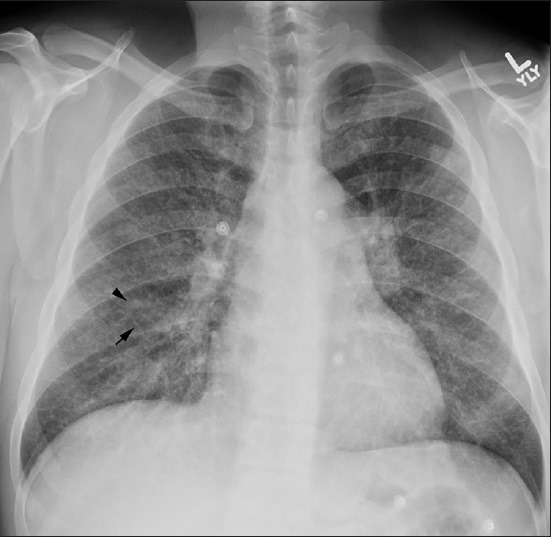
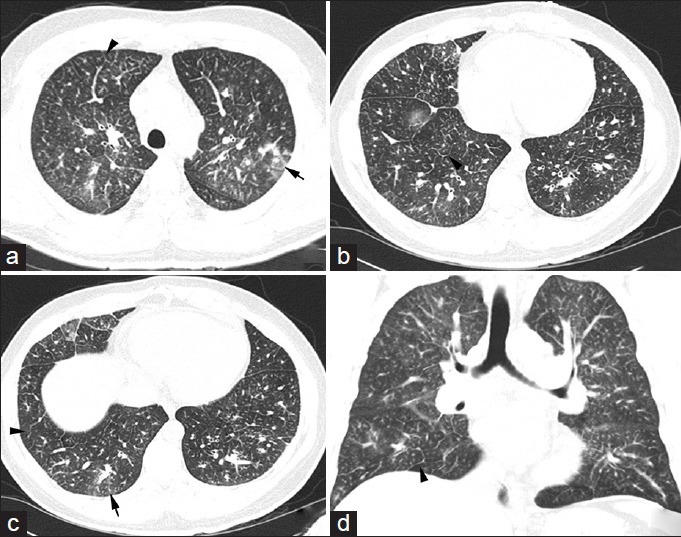
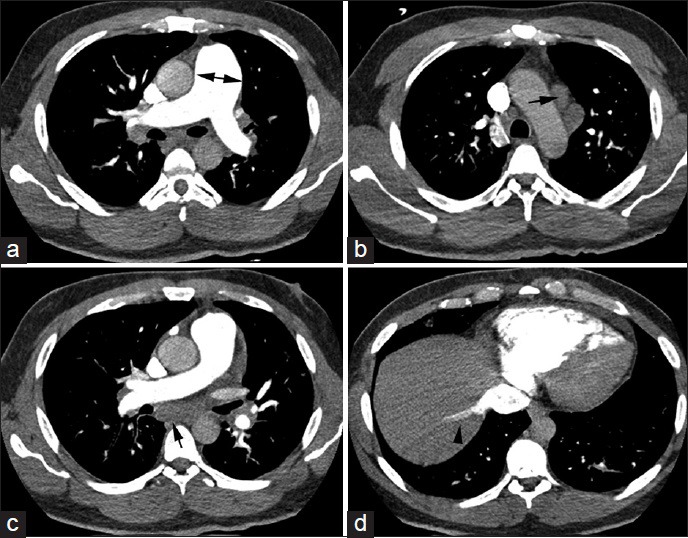
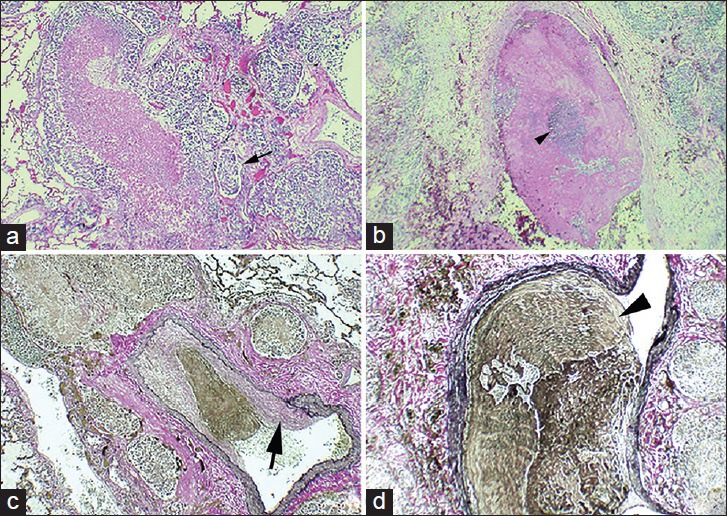
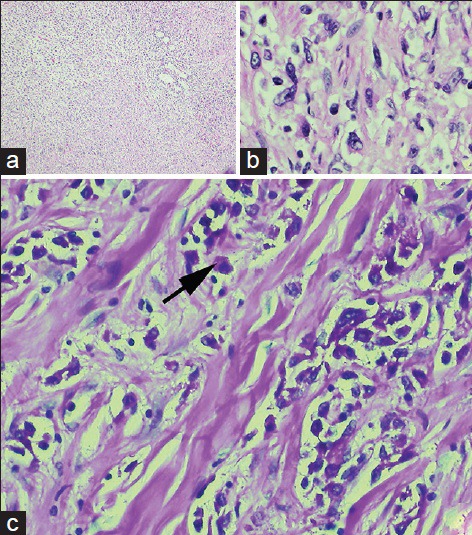
Pulmonary tumor thrombotic microangiopathy (PTTM) is a clinicopathologic disease entity in which the tumor cells embolize to the pulmonary vasculature leading to a series of maladaptive reactions including the activation of coagulation and fibrocellular intimal thickening. The resultant stenosis of blood vessels leads to pulmonary hypertension and eventual death from cor pulmonale. In this report, we present a case of PTTM presenting as the initial manifestation of metastatic gastric carcinoma in a young man. Although unusual in its occurrence as the initial manifestation of gastric carcinoma, the case is illustrative in its clinical, radiological and histological presentation.
Keywords: Cancer; embolism; pulmonary hypertension.
Figures
References
-
- von Herbay A, Illes A, Waldherr R, Otto HF. Pulmonary tumor thrombotic microangiopathy with pulmonary hypertension. Cancer. 1990;66:587–92. - PubMed
-
- Chinen K, Tokuda Y, Masachika F, Fujioka Y. Pulmonary tumor thrombotic microangiopathy in patients with gastric carcinoma: An analysis of 6 autopsy cases and review of the literature. Pathol Res Pract. 2010;206:682–9. - PubMed
-
- Kayatani H, Matsuo K, Ueda Y, Matsushita M, Fujiwara K, Yonei T, et al. Pulmonary tumor thrombotic microangiopathy diagnosed antemortem and treated with combination chemotherapy. Intern Med. 2012;51:2767–70. - PubMed
-
- Miyano S, Izumi S, Takeda Y, Tokuhara M, Mochizuki M, Matsubara O, et al. Pulmonary tumor thrombotic microangiopathy. J Clin Oncol. 2007;25:597–9. - PubMed
-
- Franquet T, Giménez A, Prats R, Rodríguez-Arias JM, Rodríguez C. Thrombotic microangiopathy of pulmonary tumors: A vascular cause of tree-in-bud pattern on CT. AJR Am J Roentgenol. 2002;179:897–9. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources