

Integrated Simulation Framework for Toxicity, Dose Intensity, Disease Progression, and Cost Effectiveness for Castration-Resistant Prostate Cancer Treatment With Eribulin
- PMID: 26312161
- PMCID: PMC4544051
- DOI: 10.1002/psp4.48
Integrated Simulation Framework for Toxicity, Dose Intensity, Disease Progression, and Cost Effectiveness for Castration-Resistant Prostate Cancer Treatment With Eribulin
Abstract
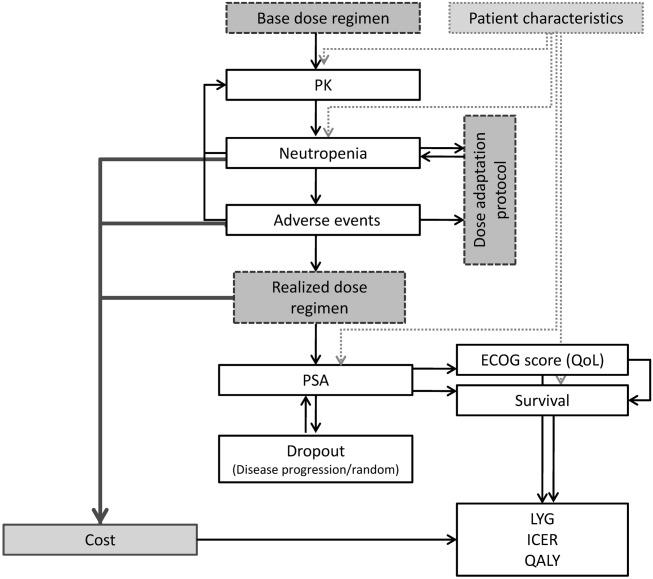
Quantitative model-based analyses are helpful to support decision-making in drug development. In oncology, disease progression/clinical outcome (DPCO) models have been used for early predictions of clinical outcome, but most of such approaches did not include adverse events or dose intensity. In addition, cost-effectiveness evaluations of investigational compounds are becoming increasingly important. Here, we developed an integrated model-based framework including relevant treatment effects for patients with castration-resistant prostate cancer treated with the anticancer agent eribulin. The framework included (i) a DPCO model relating prostate-specific antigen (PSA) dynamics to survival; (ii) models for adverse events including dose-limiting neutropenia and other graded toxicities; (iii) a model for Eastern Cooperative Oncology Group (ECOG) performance score; (iv) a model for dropout; (v) the consideration of cost effectiveness. The model allowed simulation of realistic treatment courses. Subsequently, simulations evaluating alternative treatment protocols or patient characteristics were performed in order to derive inferences on expected efficacy and cost effectiveness.
Figures
References
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
