

Albumin Kinetics in Patients Undergoing Major Abdominal Surgery
- PMID: 26313170
- PMCID: PMC4552033
- DOI: 10.1371/journal.pone.0136371
Albumin Kinetics in Patients Undergoing Major Abdominal Surgery
Abstract
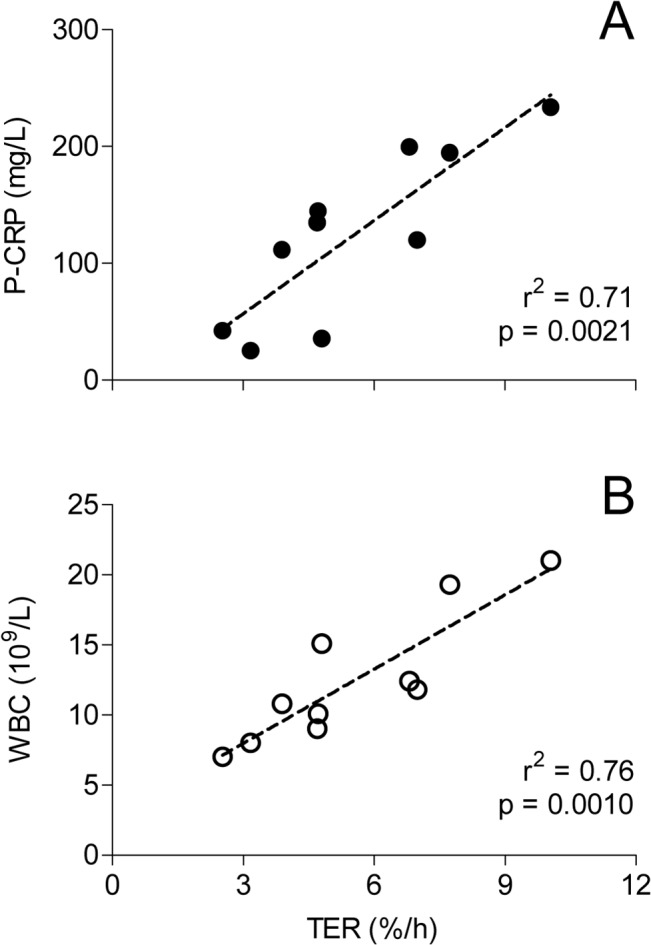
Background: The drop in plasma albumin concentration following surgical trauma is well known, but the temporal pattern of the detailed mechanisms behind are less well described. The aim of this explorative study was to assess changes in albumin synthesis and transcapillary escape rate (TER) following major surgical trauma, at the time of peak elevations in two well-recognized markers of inflammation.
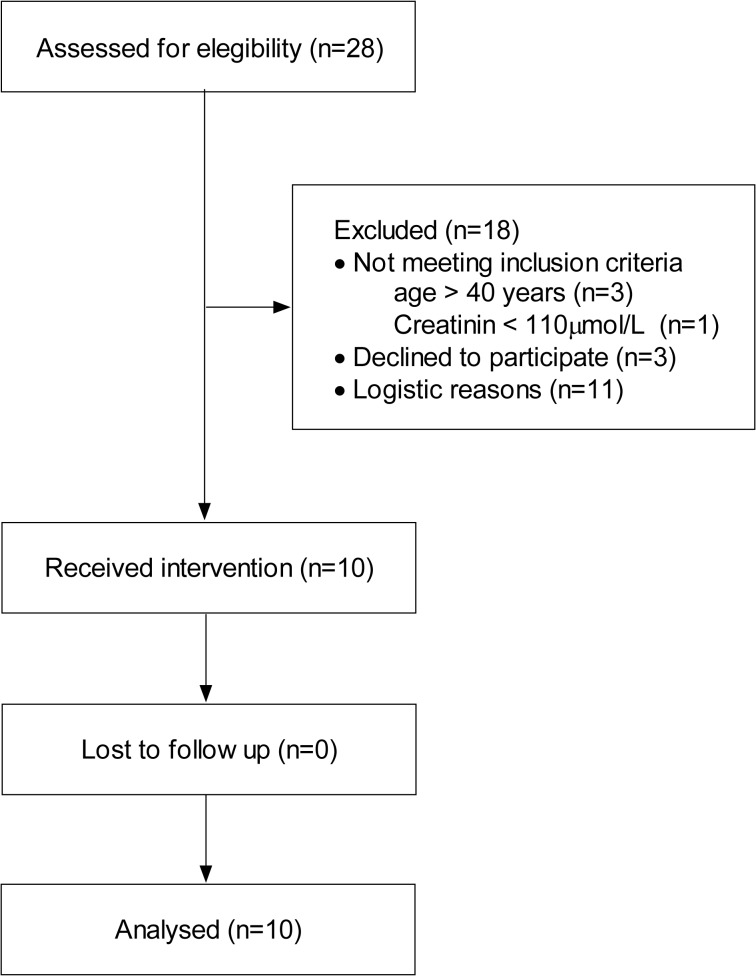
Methods: This was a clinical trial of radiolabeled human serum albumin for the study of TER and plasma volume. Ten patients were studied immediately preoperatively and on the 2nd postoperative day after major pancreatic surgery. Albumin synthesis rate was measured by the flooding dose technique employing incorporation of isotopically labelled phenylalanine.
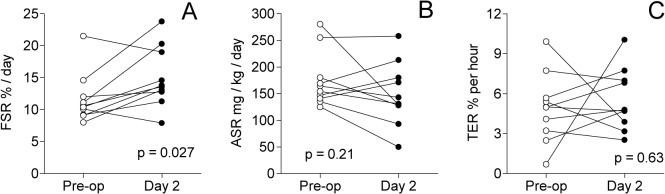
Results: Fractional synthesis rate of albumin increased from 11.7 (95% CI: 8.9, 14.5) to 15.0 (11.7, 18.4) %/day (p = 0.027), whereas the corresponding absolute synthesis rate was unchanged, 175 (138, 212) versus 150 (107, 192) mg/kg/day (p = 0.21). TER was unchanged, 4.9 (3.1, 6.8) %/hour versus 5.5 (3.9, 7.2) (p = 0.63). Plasma volume was unchanged but plasma albumin decreased from 33.5 (30.9, 36.2) to 22.1 (19.8, 24.3) g/L. (p<0.001).
Conclusion: Two days after major abdominal surgery, at the time-point when two biomarkers of generalised inflammation were at their peak and the plasma albumin concentration had decreased by 33%, we were unable to show any difference in the absolute synthesis rate of albumin, TER and plasma volume as compared with values obtained immediately pre-operatively. This suggests that capillary leakage, if elevated postoperatively, had ceased at that time-point. The temporal relations between albumin kinetics, capillary leakage and generalised inflammation need to be further explored.
Trial registration: clinicaltrialsregister.eu: EudraCT 2010-08529-21 ClinicalTrials.gov NCT01194492.
Conflict of interest statement
Figures

References
-
- Yates DR, Davies SJ, Milner HE, Wilson RJ. Crystalloid or colloid for goal-directed fluid therapy in colorectal surgery. Br J Anaesth. 2013. - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
