

Who Gets Early Tracheostomy?: Evidence of Unequal Treatment at 185 Academic Medical Centers
- PMID: 26313324
- PMCID: PMC4631039
- DOI: 10.1378/chest.15-0576
Who Gets Early Tracheostomy?: Evidence of Unequal Treatment at 185 Academic Medical Centers
Abstract
Background: Although the benefits of early tracheostomy in patients dependent on ventilators are well established, the reasons for variation in time from intubation to tracheostomy remain unclear. We identified clinical and demographic disparities in time to tracheostomy.
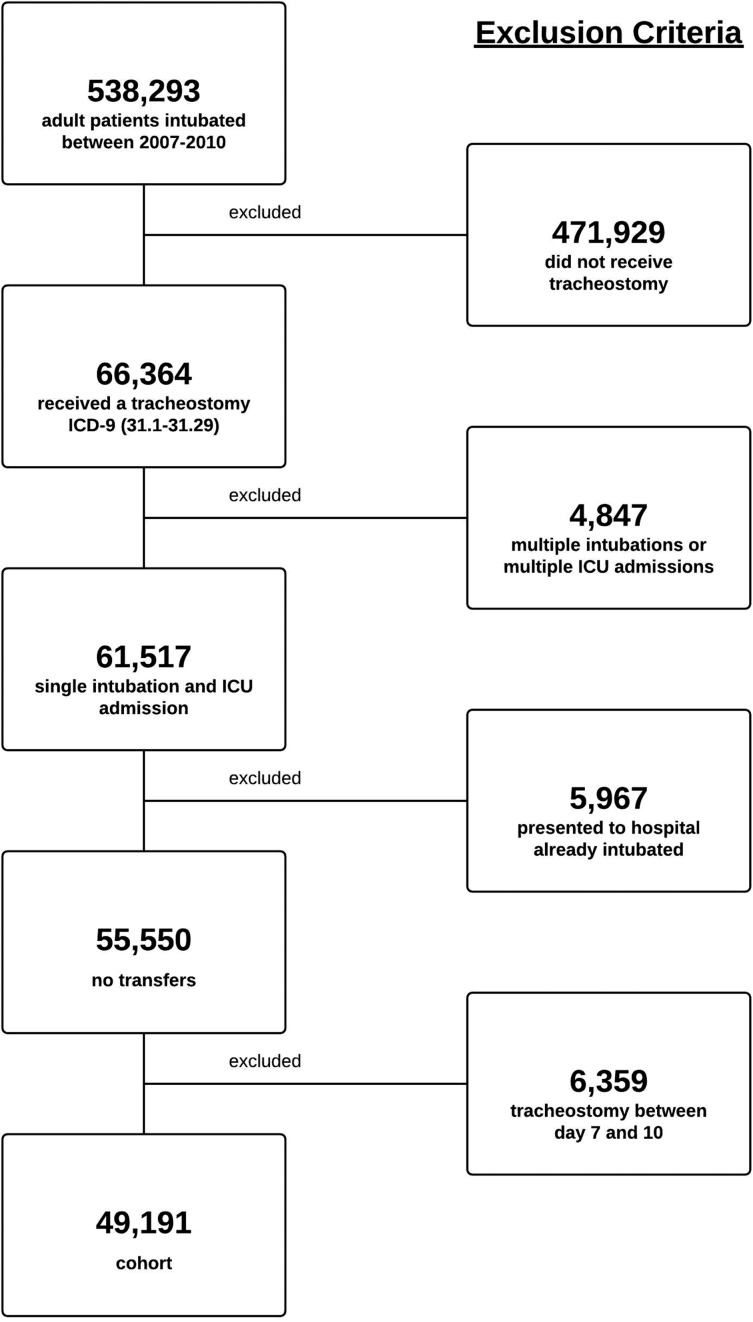
Methods: We performed a level 3 retrospective prognostic study by querying the University HealthSystem Consortium (2007-2010) for adult patients receiving a tracheostomy after initial intubation. Time to tracheostomy was designated early (< 7 days) or late (> 10 days). Cohorts were stratified by time to tracheostomy and compared using univariate tests of association and multivariable adjusted models.
Results: A total of 49,191 patients underwent tracheostomy after initial intubation: 42% early (n = 21,029) and 58% late (n = 28,162). On both univariate and multivariable analyses, women, blacks, Hispanics, and patients receiving Medicaid were less likely to receive an early tracheostomy. Patients in the early group also experienced lower rates of mortality (OR, 0.84; 95% CI, 0.79-0.88).
Conclusions: Early tracheostomy was associated with increased survival. Yet, there were still significant disparities in time to tracheostomy according to sex, race, and type of insurance. Application of evidence-based algorithms for tracheostomy may reduce unequal treatment and improve overall mortality rates. Additional research into this apparent bias in referral/rendering of tracheostomy is needed.
Figures
References
-
- Healthcare Cost and Utilization Project (HCUP). 2006-2009. Agency for Healthcare Research and Quality website. http://hcupnet.ahrq.gov/. Accessed January 31, 2013. - PubMed
-
- Walts PA, Murthy SC, DeCamp MM. Techniques of surgical tracheostomy. Clin Chest Med. 2003;24(3):413-422. - PubMed
-
- Wang HK, et al. The impact of tracheostomy timing in patients with severe head injury: an observational cohort study. Injury. 2012;43(9):1432-1436. - PubMed
-
- Van Bommel J, Van der Hoven B. Tracheostomy in the ICU: is timing everything? Minerva Anestesiol. 2010;76(3):171-172. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
