

Escitalopram pharmacogenetics: CYP2C19 relationships with dosing and clinical outcomes in autism spectrum disorder
- PMID: 26313485
- PMCID: PMC4591203
- DOI: 10.1097/FPC.0000000000000173
Escitalopram pharmacogenetics: CYP2C19 relationships with dosing and clinical outcomes in autism spectrum disorder
Abstract
Background and aim: Selective serotonin reuptake inhibitors such as escitalopram are commonly used to treat patients with autism spectrum disorder (ASD), but there are individual differences in treatment response and tolerability. CYP2C19 encodes the primary enzyme responsible for escitalopram metabolism and we investigated whether polymorphisms in CYP2C19 were related to symptoms and dosing in a pharmacogenetic study of ASD.
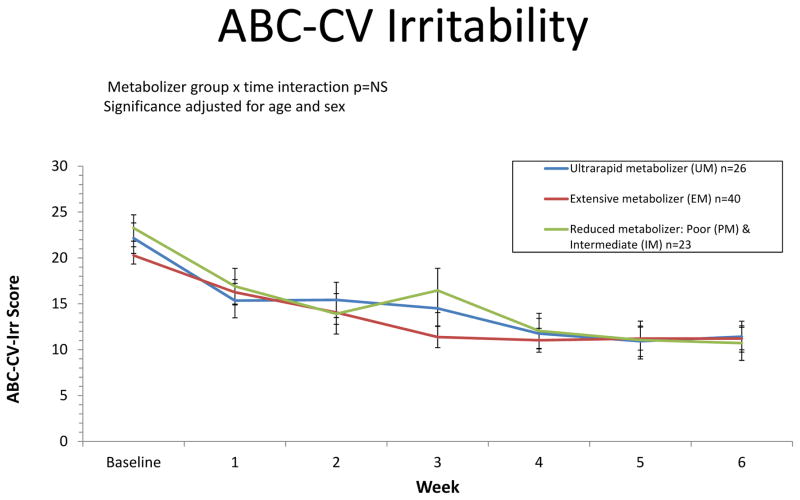
Participants and methods: Participants completed the Aberrant Behavior Checklist--Community Version (ABC-CV) weekly for 6 weeks. Escitalopram was initiated at a dose of 2.5 mg per day, with weekly increases to 20 mg unless intolerable side-effects occurred. Three CYP2C19 metabolizer groups, including ultrarapid, extensive, and reduced metabolizers, were examined in relation to symptom improvement and tolerated dose.
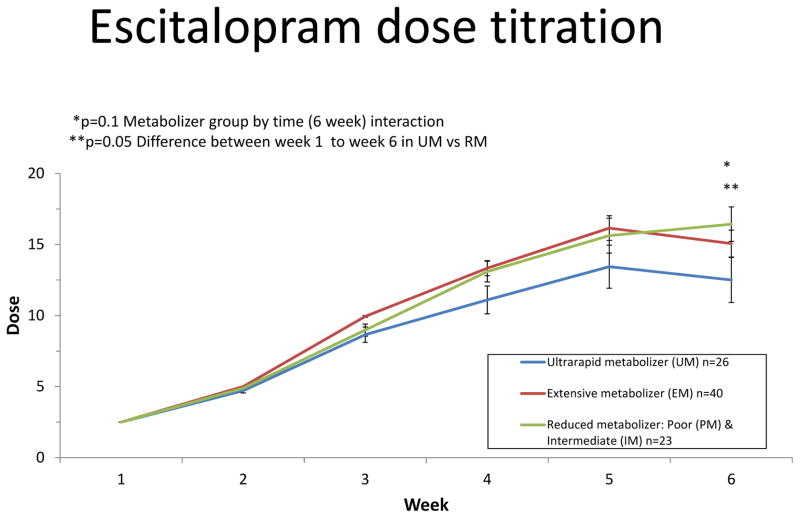
Results: ABC-CV scores improved over the course of treatment (P<0.0001). No differences were identified in the rate of improvement across metabolizer groups for the ABC-CV irritability subscale, which was the primary outcome for clinical symptoms. There was a trend for a metabolizer group by time interaction with respect to dose (P=0.10). This interaction was driven by the linear rate of change from week 1 to study endpoint between the reduced metabolizers and ultrarapid metabolizer groups (P=0.05). Post-hoc analyses identified significant differences in the rate of dose escalation between ultrarapid metabolizers and extensive metabolizers and for ultrarapid metabolizers compared with reduced metabolizers (P's<0.04), whereby ultrarapid metabolizers showed a slower rate of change in dose over time.
Conclusion: CYP2C19 ultrarapid metabolizers were associated with reduced tolerance to a fixed titration schedule of open-label escitalopram in this ASD study sample. Possible explanations may involve the altered kinetics of faster metabolizers or previously unknown activities of escitalopram metabolites.
Conflict of interest statement
J.R.B is on a scientific advisory board for Physician’s Choice Laboratory Services and Ortho-McNeil Janssen, E.H.C has been a consultant for a Seaside Therapeutics multi-site clinical trial. SJ serves as a part of a Roche Pharmaceuticals multi-site clinical trial. The remaining authors report no disclosures.
Figures
References
-
- Association AP. Diagnostic and Statistical Manual of Mental Disorders. 4. Washington, DC: American Psychiatric Association; 2000. Text Revision: DSM-IV-TR.
-
- Association AP. Diagnostic and Statistical Manual of Mental Disorders. 5. Washington, D.C: American Psychiatric Association; 2013. DSM-5.
-
- CDC. Prevalence of autism spectrum disorder among children aged 8 years - autism and developmental disabilities monitoring network, 11 sites, United States, 2010. Morbidity and mortality weekly report Surveillance summaries (Washington, DC: 2002) 2014;63(2):1–21. - PubMed
-
- Volkmar F, Siegel M, Woodbury-Smith M, King B, McCracken J, State M. Practice parameter for the assessment and treatment of children and adolescents with autism spectrum disorder. J Am Acad Child Adolesc Psychiatry. 2014;53(2):237–57. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- K23092696/PHS HHS/United States
- K23 MH082121/MH/NIMH NIH HHS/United States
- K01MH098798/MH/NIMH NIH HHS/United States
- NIMH P50MH094267/PHS HHS/United States
- K08 MH083888/MH/NIMH NIH HHS/United States
- P50 MH094267/MH/NIMH NIH HHS/United States
- NIEHS P50HD055751/HD/NICHD NIH HHS/United States
- K23MH082121/MH/NIMH NIH HHS/United States
- K01MH064539/MH/NIMH NIH HHS/United States
- P50 HD055751/HD/NICHD NIH HHS/United States
- K08MH083888/MH/NIMH NIH HHS/United States
- K01 MH098798/MH/NIMH NIH HHS/United States
- K01 MH064539/MH/NIMH NIH HHS/United States
