

Aggressive spinal haemangiomas: imaging correlates to clinical presentation with analysis of treatment algorithm and clinical outcomes
- PMID: 26313498
- PMCID: PMC4743441
- DOI: 10.1259/bjr.20140771
Aggressive spinal haemangiomas: imaging correlates to clinical presentation with analysis of treatment algorithm and clinical outcomes
Abstract
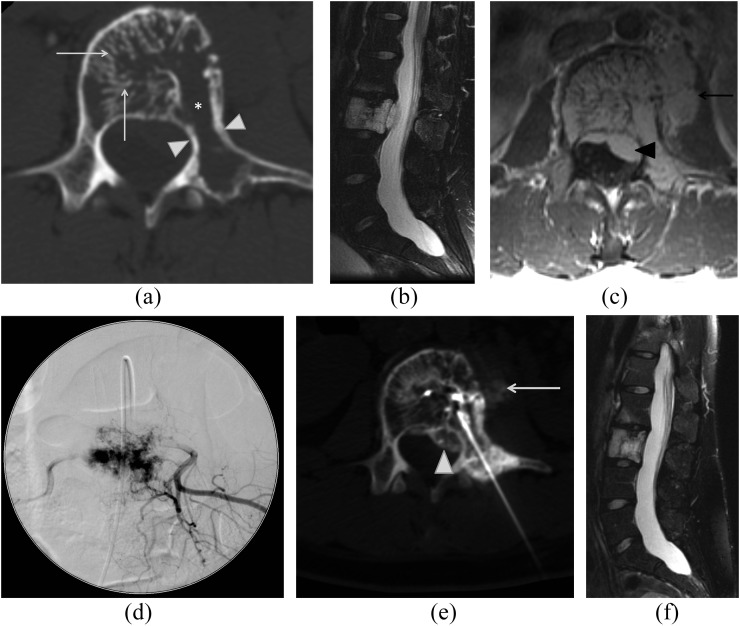
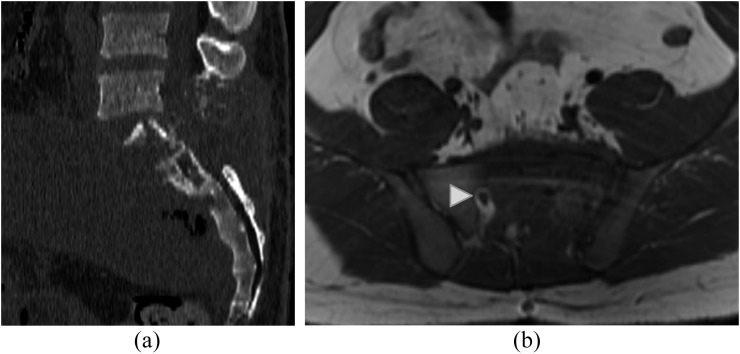
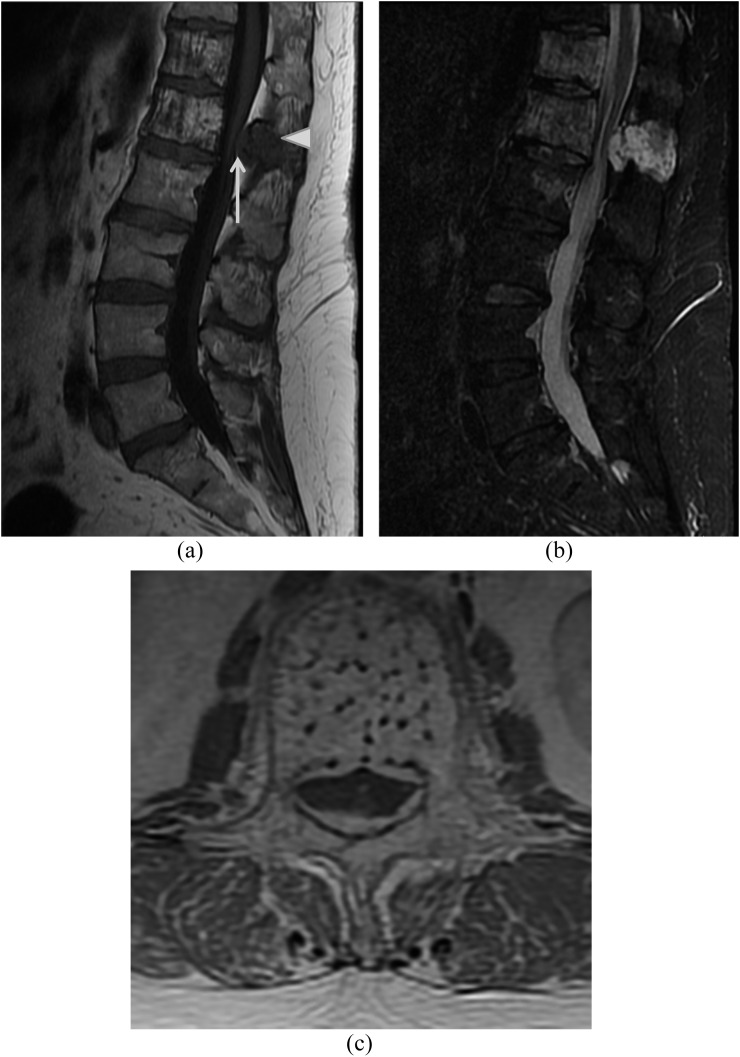
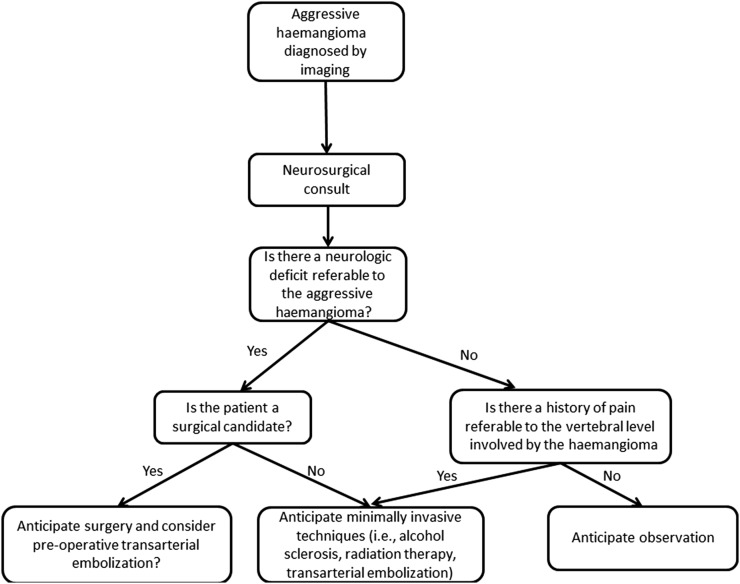
Objective: Aggressive spinal haemangiomas (those with significant osseous expansion/extraosseous extension) represent approximately 1% of spinal haemangiomas and are usually symptomatic. In this study, we correlate imaging findings with presenting symptomatology, review treatment strategies and their outcomes and propose a treatment algorithm.
Methods: 16 patients with aggressive haemangiomas were retrospectively identified from 1995 to 2013. Imaging was assessed for size, location, CT/MR characteristics, osseous expansion and extraosseous extension. Presenting symptoms, management and outcomes were reviewed.
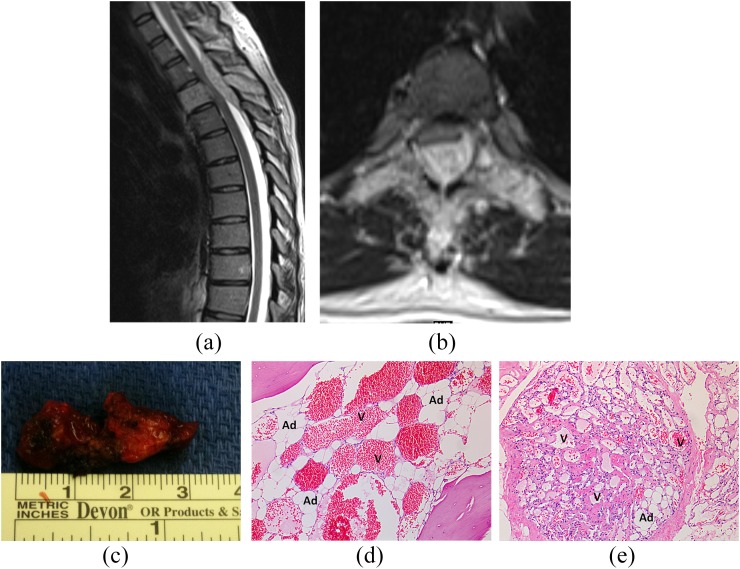
Results: Median patient age was 52 years. Median size was 4.5 cm. Lumbar spine was the commonest location (n = 8), followed by thoracic spine (n = 7) and sacrum (n = 2); one case involved the lumbosacral junction. 12 haemangiomas had osseous expansion; 13 had extraosseous extension [epidural (n = 11), pre-vertebral/paravertebral (n = 10) and foraminal (n = 6)]. On CT, 11 had accentuated trabeculae and 5 showed lysis. On MRI, eight were T1 hyperintense, six were T1 hypointense and all were T2 hyperintense. 11 symptomatic patients underwent treatment: chemical ablation (n = 6), angioembolization (n = 3, 2 had subsequent surgery), radiotherapy (n = 2, 1 primary and 1 adjuvant) and surgery (n = 4). Median follow-up was 20 months. Four of six patients managed only by percutaneous methods had symptom resolution. Three of four patients requiring surgery had symptom resolution.
Conclusion: Aggressive haemangiomas cause significant morbidity. Treatment is multidisciplinary, with surgery reserved for large lesions and those with focal neurological signs. Minimally invasive procedures may be successful in smaller lesions.
Advances in knowledge: Aggressive haemangiomas are rare, but knowledge of their imaging features and treatment strategies enhances the radiologist's role in their management.
Figures
References
-
- Dagi TF, Schmidek HH. Vascular tumors of the spine. In: Sundaresan N, Schmidek HH, Schiller AL, et al. , eds. Tumors of the spine: diagnosis and clinical management. Philadelphia, PA: WB Saunders Co.; 1990. pp. 181–91.
-
- Murphey MD, Fairbairn KJ, Parman LM, Baxter KG, Parsa MB, Smith WS. Musculoskeletal angiomatous lesions: radiologic-pathologic correlation. Radiographics 1995; 15: 893–917. - PubMed
-
- Alexander J, Meir A, Vrodos N, Yau YH. Vertebral hemangioma: an important differential in the evaluation of locally aggressive spinal lesions. Spine (Phila Pa 1976) 2010; 35: E917–20. - PubMed
-
- Yousem DM, Grossman RI. Nondegenerative disease of the spine. In: Yousem DM, Grossman RI, eds. Neuroradiology: the requisites. Philadelphia, PA: Mosby, Inc.; 2010. pp. 543–86.
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
