

Ultrasound-guided interventional procedures around the shoulder
- PMID: 26313499
- PMCID: PMC4985952
- DOI: 10.1259/bjr.20150372
Ultrasound-guided interventional procedures around the shoulder
Abstract
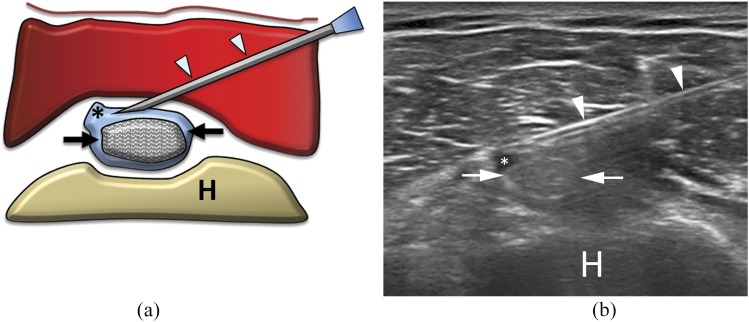
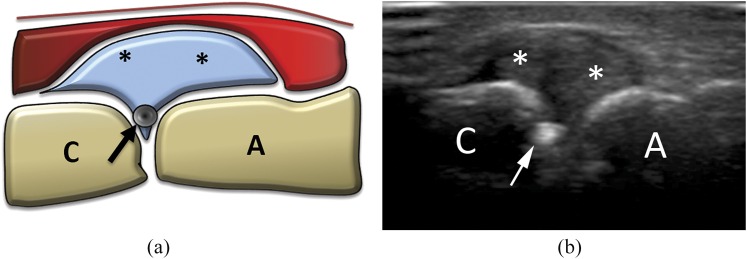
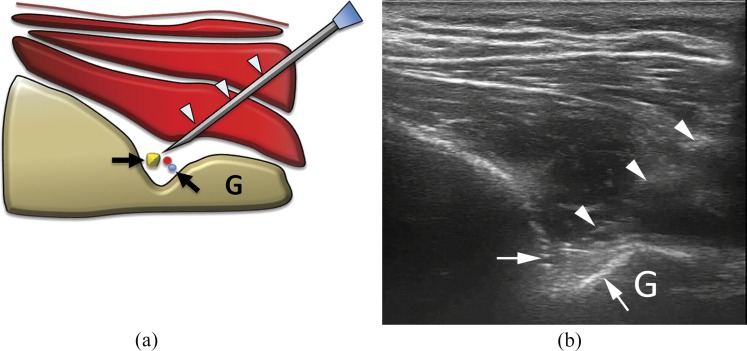
Ultrasound is an established modality for shoulder evaluation, being accurate, low cost and radiation free. Different pathological conditions can be diagnosed using ultrasound and can be treated using ultrasound guidance, such as degenerative, traumatic or inflammatory diseases. Subacromial-subdeltoid bursitis is the most common finding on ultrasound evaluation for painful shoulder. Therapeutic injections of corticosteroids are helpful to reduce inflammation and pain. Calcific tendinopathy of rotator cuff affects up to 20% of painful shoulders. Ultrasound-guided treatment may be performed with both single- and double-needle approach. Calcific enthesopathy, a peculiar form of degenerative tendinopathy, is a common and mostly asymptomatic ultrasound finding; dry needling has been proposed in symptomatic patients. An alternative is represented by autologous platelet-rich plasma injections. Intra-articular injections of the shoulder can be performed in the treatment of a variety of inflammatory and degenerative diseases with corticosteroids or hyaluronic acid respectively. Steroid injections around the long head of the biceps brachii tendon are indicated in patients with biceps tendinopathy, reducing pain and humeral tenderness. The most common indication for acromion-clavicular joint injection is degenerative osteoarthritis, with ultrasound representing a useful tool in localizing the joint space and properly injecting various types of drugs (steroids, lidocaine or hyaluronic acid). Suprascapular nerve block is an approved treatment for chronic shoulder pain non-responsive to conventional treatments as well as candidate patients for shoulder arthroscopy. This review provides an overview of these different ultrasonography-guided procedures that can be performed around the shoulder.
Figures
References
-
- Sconfienza LM, Serafini G, Silvestri E, eds. Ultrasound-guided musculoskeletal procedures: the upper Limb. Milan, Italy: Springer-Verlag; 2012.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
