

Primary Pulmonary Synovial Sarcoma in a Tertiary Referral Center: Clinical Characteristics, CT, and 18F-FDG PET Findings, With Pathologic Correlations
- PMID: 26313782
- PMCID: PMC4602937
- DOI: 10.1097/MD.0000000000001392
Primary Pulmonary Synovial Sarcoma in a Tertiary Referral Center: Clinical Characteristics, CT, and 18F-FDG PET Findings, With Pathologic Correlations
Abstract
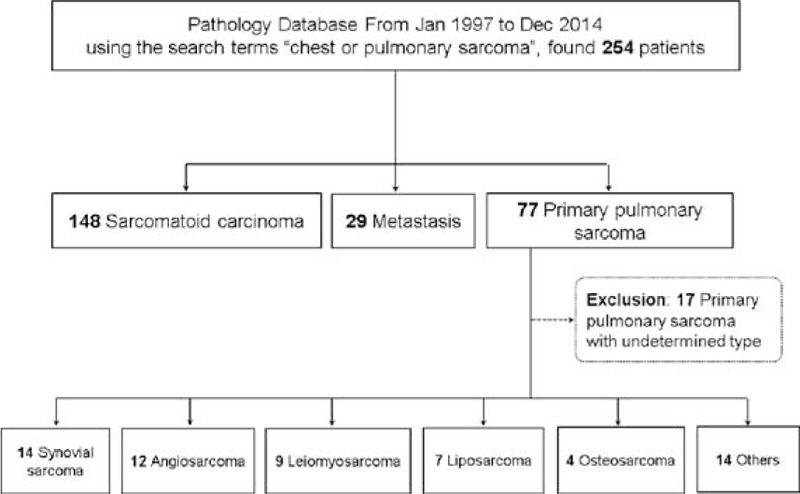
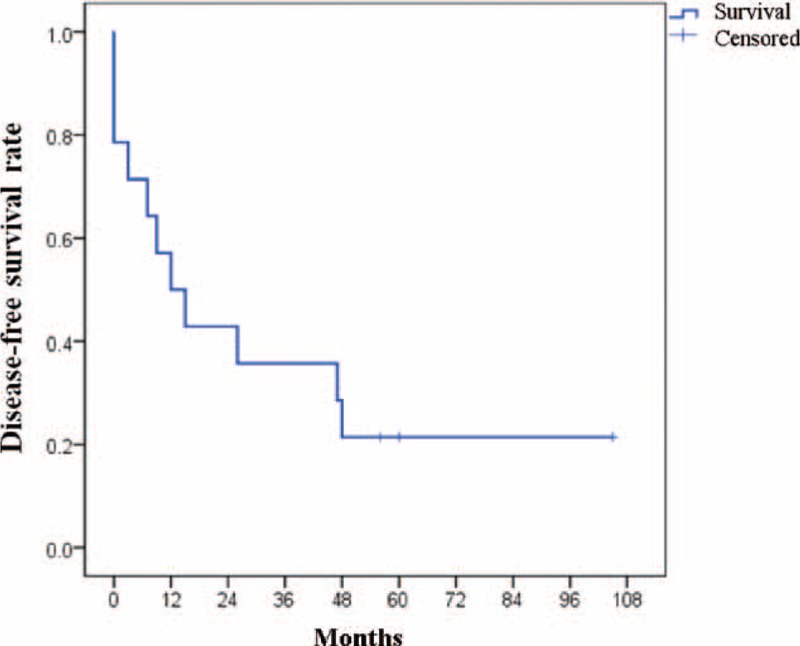
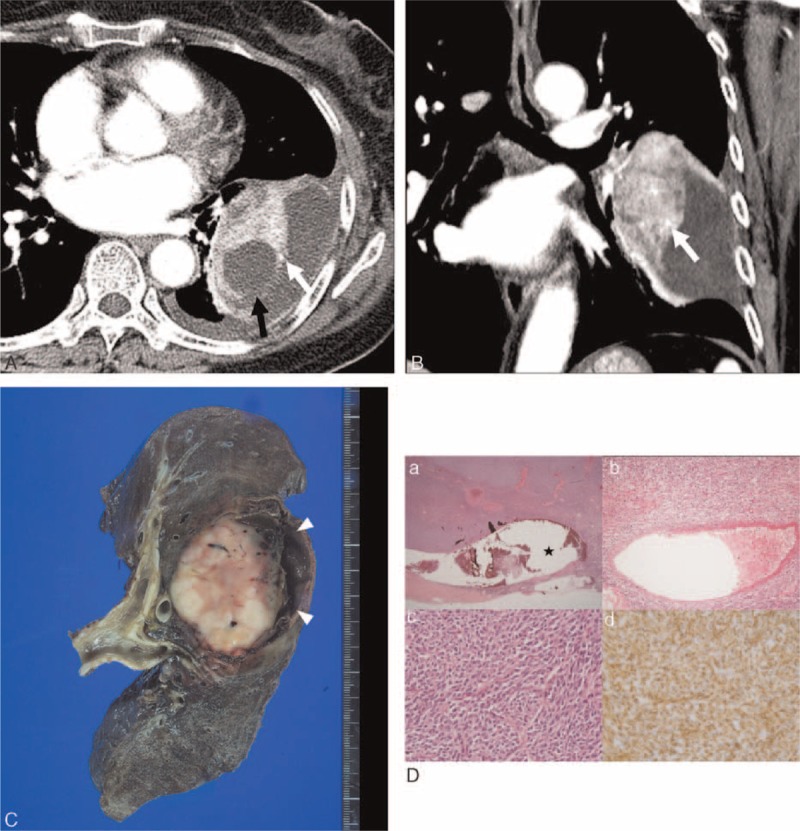
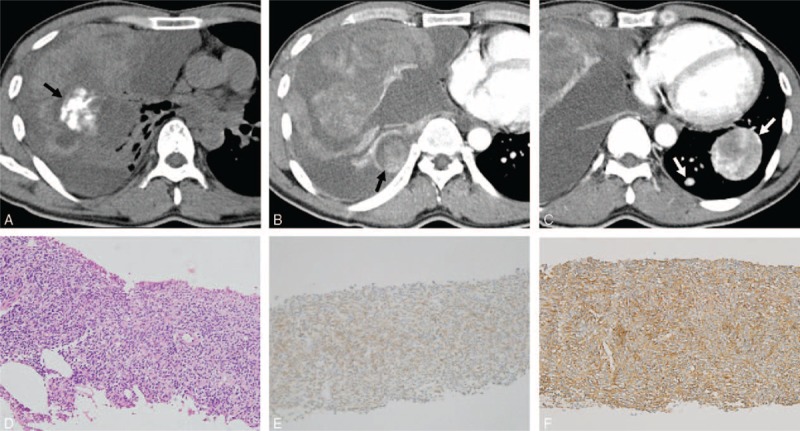
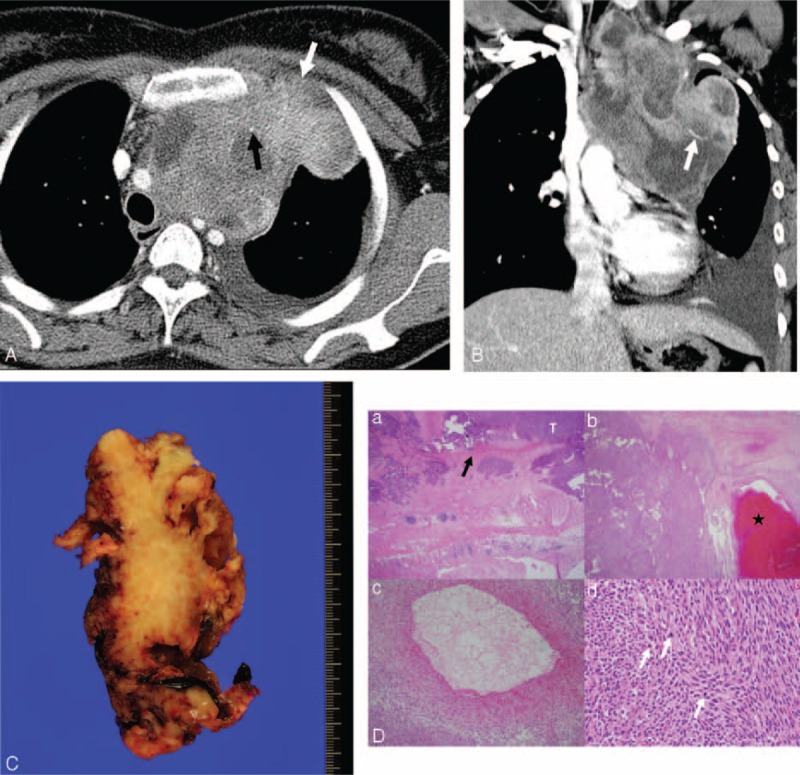
The purpose of this study was to describe the patient characteristics, computed tomography (CT) and F-fluorodeoxyglucose positron emission tomography (FDG PET) findings, and clinical outcomes of primary pulmonary synovial sarcoma (PPSS), together with their pathologic correlations. The medical records of 14 patients with pathologically proven PPSS in a tertiary hospital from January 1997 to December 2014 were retrospectively reviewed. The CT findings were evaluated. The maximum standardized uptake value (maxSUV) of the tumors was obtained, and clinical outcomes with respect to tumor recurrence and mortality were assessed by Kaplan-Meier analysis. The median tumor size was 10.2 cm and the most common anatomic location was the lung followed by the pleura/chest wall and mediastinum. Most of the tumors appeared as single lesions and had circumscribed margins. All the cases showed heterogeneous enhancement with necrotic or cystic portions, and intratumoral vessels were frequently seen. Half of the tumors had intratumoral calcifications, and tumor rupture, pleural/chest wall extension, and pleural effusion occurred frequently. However, lymph node enlargement was rare. The median maxSUV of the tumors was 4.35. Patient outcomes with respect to tumor recurrence (n = 8, 57.1%) and death (n = 3, 21.4%) were poor despite their young age, and the mean follow-up period was 28.5 months.In conclusion, PPSS usually occurs in young adults, generally in the lung, presents as a large, circumscribed mass, and tumor rupture or extension of the pleura/chest wall may occur. The tumors often contain calcifications and vessels; they may exhibit triple attenuation on enhanced CT images, and clinical outcomes are poor.
Conflict of interest statement
The authors have no funding and conflicts of interest to disclose.
Figures
References
-
- Hartel PH, Fanburg-Smith JC, Frazier AA, et al. Primary pulmonary and mediastinal synovial sarcoma: a clinicopathologic study of 60 cases and comparison with five prior series. Mod Pathol 2007; 20:760–769. - PubMed
-
- Zeren H, Moran CA, Suster S, et al. Primary pulmonary sarcomas with features of monophasic synovial sarcoma: a clinicopathological, immunohistochemical, and ultrastructural study of 25 cases. Hum Pathol 1995; 26:474–480. - PubMed
-
- Keel SB, Bacha E, Mark EJ, et al. Primary pulmonary sarcoma: a clinicopathologic study of 26 cases. Mod Pathol 1999; 12:1124–1131. - PubMed
-
- Frazier AA, Franks TJ, Pugatch RD, et al. From the archives of the AFIP: pleuropulmonary synovial sarcoma. Radiographics 2006; 26:923–940. - PubMed
-
- Raney RB. Synovial sarcoma in young people: background, prognostic factors, and therapeutic questions. J Pediatr Hematol/Oncol 2005; 27:207–211. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
