

Repetitive Transcranial Magnetic Stimulation (rTMS) Therapy in Parkinson Disease: A Meta-Analysis
- PMID: 26314233
- PMCID: PMC5540142
- DOI: 10.1016/j.pmrj.2015.08.009
Repetitive Transcranial Magnetic Stimulation (rTMS) Therapy in Parkinson Disease: A Meta-Analysis
Abstract
Objective: Several studies have reported repetitive transcranial magnetic stimulation (rTMS) therapy as an effective treatment for the control of motor symptoms in Parkinson disease. The objective of the study is to quantify the overall efficacy of this treatment.
Types: Systematic review and meta-analysis.
Literature survey: We reviewed the literature on clinical rTMS trials in Parkinson disease since the technique was introduced in 1980. We used the following databases: MEDLINE, Web of Science, Cochrane, and CINAHL.
Patients and setting: Patients with Parkinson disease who were participating in prospective clinical trials that included an active arm and a control arm and change in motor scores on Unified Parkinson's Disease Rating Scale as the primary outcome. We pooled data from 21 studies that met these criteria. We then analyzed separately the effects of low- and high-frequency rTMS on clinical motor improvements.
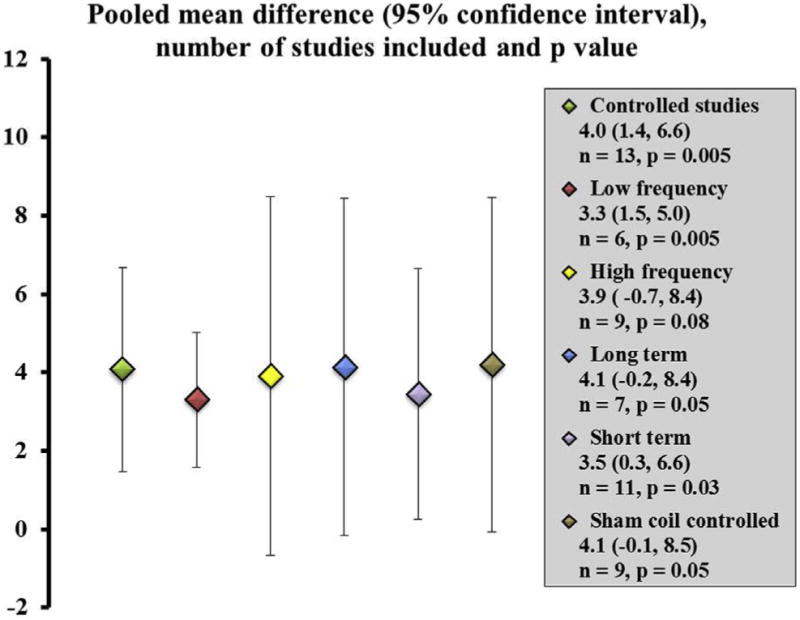
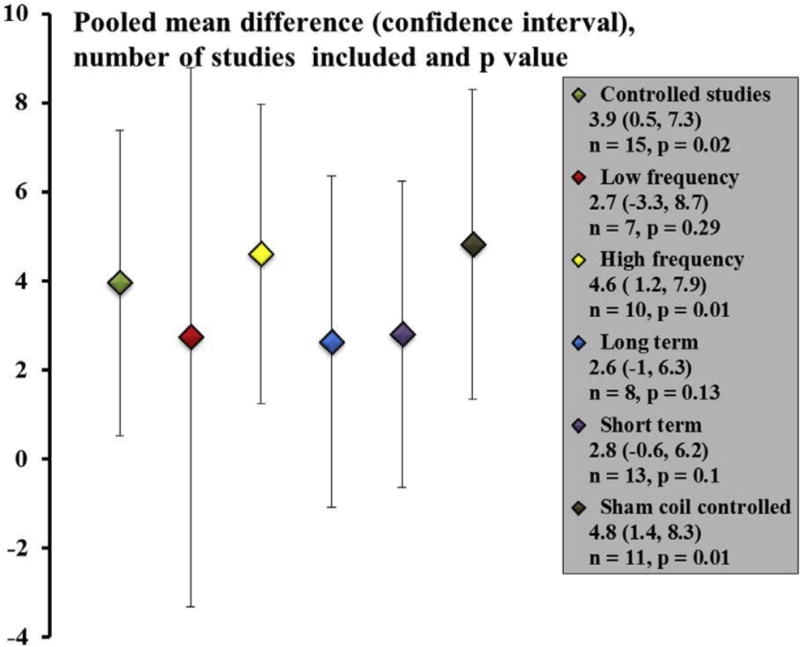
Synthesis: The overall pooled mean difference between treatment and control groups in the Unified Parkinson's Disease Rating Scale motor score was significant (4.0 points, 95% confidence interval, 1.5, 6.7; P = .005). rTMS therapy was effective when low-frequency stimulation (≤ 1 Hz) was used with a pooled mean difference of 3.3 points (95% confidence interval 1.6, 5.0; P = .005). There was a trend for significance when high-frequency stimulation (≥ 5 Hz) studies were evaluated with a pooled mean difference of 3.9 points (95% confidence interval, -0.7, 8.5; P = .08). rTMS therapy demonstrated benefits at short-term follow-up (immediately after a treatment protocol) with a pooled mean difference of 3.4 points (95% confidence interval, 0.3, 6.6; P = .03) as well as at long-term follow-up (average follow-up 6 weeks) with mean difference of 4.1 points (95% confidence interval, -0.15, 8.4; P = .05). There were insufficient data to statistically analyze the effects of rTMS when we specifically examined bradykinesia, gait, and levodopa-induced dyskinesia using quantitative methods.
Conclusion: rTMS therapy in patients with Parkinson disease results in mild-to-moderate motor improvements and has the potential to be used as an adjunct therapy for the treatment of Parkinson disease. Future large, sample studies should be designed to isolate the specific clinical features of Parkinson disease that respond well to rTMS therapy.
Copyright © 2016 American Academy of Physical Medicine and Rehabilitation. Published by Elsevier Inc. All rights reserved.
Figures
References
-
- Olanow CW, Stern MB, Sethi K. The scientific and clinical basis for the treatment of Parkinson disease (2009) Neurology. 2009;72(21 Suppl 4):S1–S136. - PubMed
-
- Miyasaki JM, Martin W, Suchowersky O, Weiner WJ, Lang AE. Practice parameter: Initiation of treatment for Parkinson’s disease: An evidence-based review: report of the Quality Standards Subcommittee of the American Academy of Neurology. Neurology. 2002;58:11–17. - PubMed
-
- Okun MS, Gallo BV, Mandybur G, Jagid J, Foote KD, Revilla FJ, et al. Subthalamic deep brain stimulation with a constant-current device in Parkinson’s disease: An open-label randomised controlled trial. Lancet Neurol. 2012;11:140–149. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
