

TERT promoter mutations contribute to IDH mutations in predicting differential responses to adjuvant therapies in WHO grade II and III diffuse gliomas
- PMID: 26314843
- PMCID: PMC4694799
- DOI: 10.18632/oncotarget.4549
TERT promoter mutations contribute to IDH mutations in predicting differential responses to adjuvant therapies in WHO grade II and III diffuse gliomas
Abstract
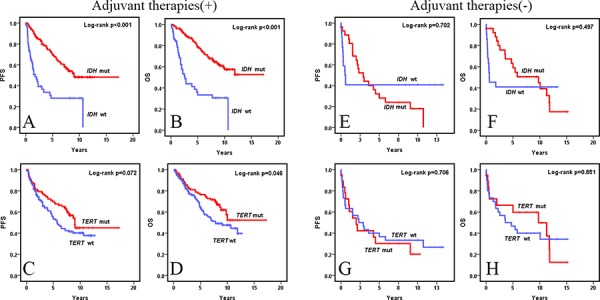
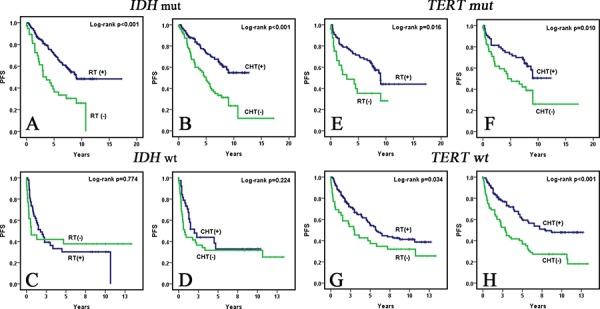
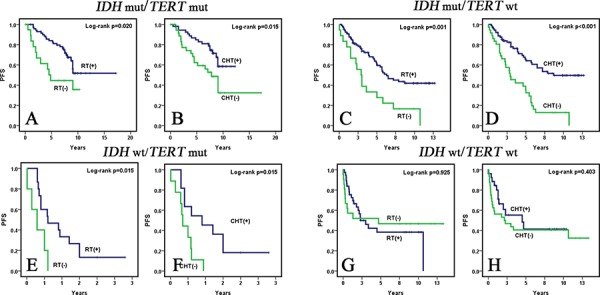
IDH mutations frequently occur in WHO grade II and III diffuse gliomas and have favorable prognosis compared to wild-type tumors. However, whether IDH mutations in WHO grade II and II diffuse gliomas predict enhanced sensitivity to adjuvant radiation (RT) or chemotherapy (CHT) is still being debated. Recent studies have identified recurrent mutations in the promoter region of telomerase reverse transcriptase (TERT) in gliomas. We previously demonstrated that TERT promoter mutations may be promising biomarkers in glioma survival prognostication when combined with IDH mutations. This study analyzed IDH and TERT promoter mutations in 295 WHO grade II and III diffuse gliomas treated with or without adjuvant therapies to explore their impact on the sensitivity of tumors to genotoxic therapies. IDH mutations were found in 216 (73.2%) patients and TERT promoter mutations were found in 112 (38%) patients. In multivariate analysis, IDH mutations (p < 0.001) were independent prognostic factors for PFS and OS in patients receiving genotoxic therapies while TERT promoter mutations were not. In univariate analysis, IDH and TERT promoter mutations were not significant prognostic factors in patients who did not receive genotoxic therapies. Adjuvant RT and CHT were factors independently impacting PFS (RT p = 0.001, CHT p = 0.026) in IDH mutated WHO grade II and III diffuse gliomas but not in IDH wild-type group. Univariate and multivariate analyses demonstrated TERT promoter mutations further stratified IDH wild-type WHO grade II and III diffuse gliomas into two subgroups with different responses to genotoxic therapies. Adjuvant RT and CHT were significant parameters influencing PFS in the IDH wt/TERT mut subgroup (RT p = 0.015, CHT p = 0.015) but not in the IDH wt/TERT wt subgroup. Our data demonstrated that IDH mutated WHO grade II and III diffuse gliomas had better PFS and OS than their IDH wild-type counterparts when genotoxic therapies were administered after surgery. Importantly, we also found that TERT promoter mutations further stratify IDH wild-type WHO grade II and III diffuse gliomas into two subgroups with different responses to adjuvant therapies. Taken together, TERT promoter mutations may predict enhanced sensitivity to genotoxic therapies in IDH wild-type WHO grade II and III diffuse gliomas and may justify intensified treatment in this subgroup.
Keywords: IDH; TERT promoter; chemotherapy; gliomas; radiation therapy.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures
References
-
- Wen PY, Kesari S. Malignant gliomas in adults. N Engl J Med. 2008;359:492–507. - PubMed
-
- Sabha N, Knobbe CB, Maganti M, Al Omar S, Bernstein M, Cairns R, Çako B, von Deimling A, Capper D, Mak TW, Kiehl TR, Carvalho P, Garrett E, et al. Analysis of IDH mutation, 1p/19q deletion, and PTEN loss delineates prognosis in clinical low-grade diffuse gliomas. Neuro Oncol. 2014;16:914–923. - PMC - PubMed
-
- Cavaliere R, Lopes MB, Schiff D. Low-grade gliomas: an update on pathology and therapy. Lancet Neurol. 2005;4:760–770. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
Miscellaneous
