

Review
doi: 10.1016/j.suc.2015.05.009.
Epub 2015 Jun 20.
Principles of Cancer Screening
Affiliations
- PMID: 26315516
- PMCID: PMC4555845
- DOI: 10.1016/j.suc.2015.05.009
Item in Clipboard
Review
Principles of Cancer Screening
Surg Clin North Am.
2015 Oct.
Abstract
Cancer screening has long been an important component of the struggle to reduce the burden of morbidity and mortality from cancer. Notwithstanding this history, many aspects of cancer screening remain poorly understood. This article presents a summary of basic principles of cancer screening that are relevant for researchers, clinicians, and public health officials alike.
Keywords: Cancer screening; Lead time; Number needed to screen; Overdiagnosis; Performance characteristics; Targeted screening.
Published by Elsevier Inc.
Figures
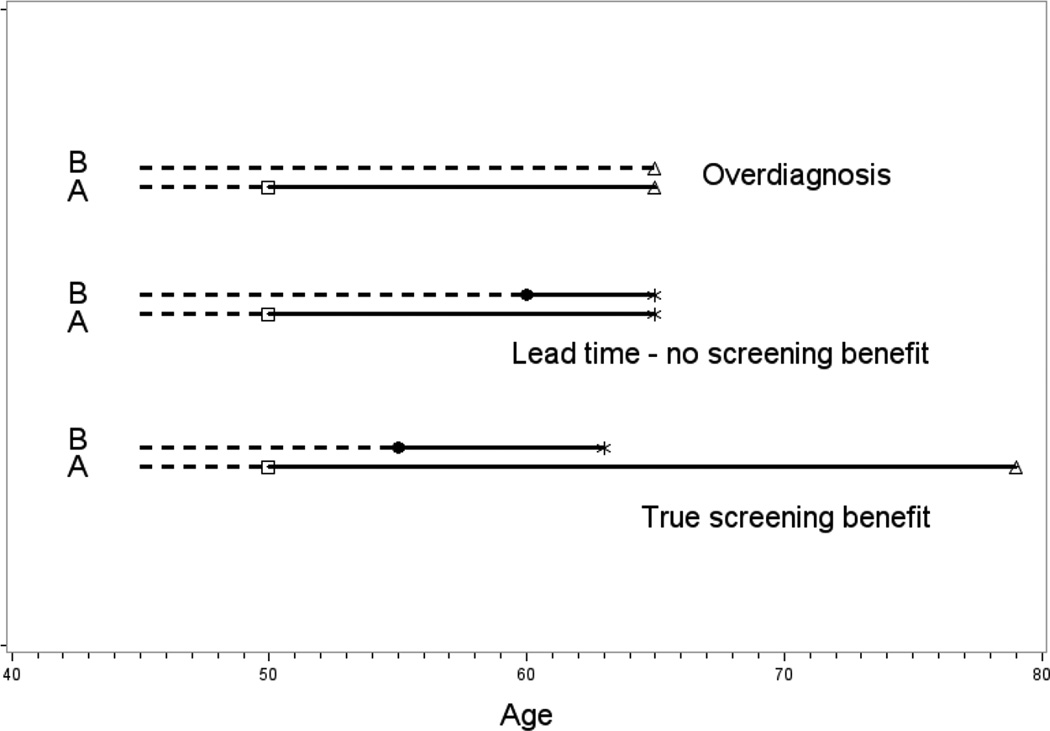
Schematic of Screening Scenarios. In each panel, A represents the scenario with screening at age 50 and B represents the hypothetical scenario if there had been no screening. Square and circle represent screen-detected and clinical diagnosis, respectively, dotted and solid line represent preclinical cancer and post-diagnosis cancer, respectively. Star and triangle denote death from the cancer of interest and death from other causes, respectively. In the lead time - no screening benefit scenario, “survival” increases from 5 to 15 years upon screening, but time and cause of death are unchanged.
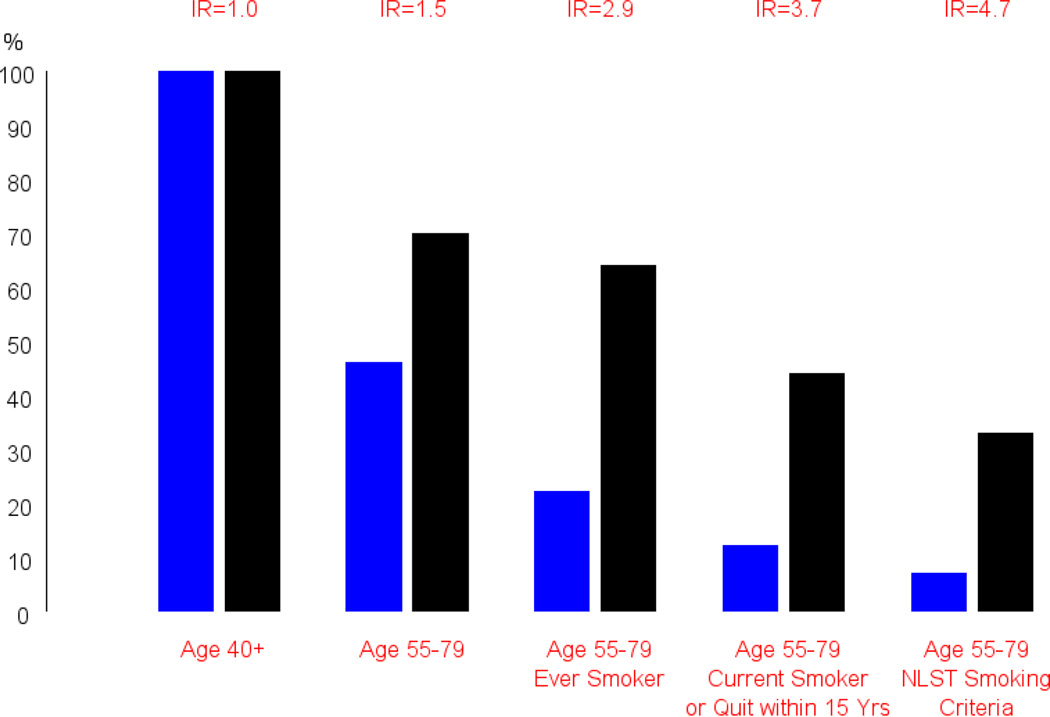
Targeted screening through risk stratification for low-dose CT lung cancer screening. Blue bars represent overall population (over age 40), black bars represent incident lung cancers. For the scenario of screening everyone over age 40 (left-most column), 100% of the population and 100% of lung cancers (in the 40+ population) are covered. With increasing age and/or smoking history requirements, the percentage of incident lung cancers covered decreases, but the percentage of the population screened decreases more sharply. The incidence ratio (IR) represents the ratio of incidence rates in the restricted population over that in the overall population; it is also the ratio of the height of the black versus blue bars. NLST smoking criteria is 30+ pack years and current smoking or quit within 15 years. (Adapted from Pinsky PF, Berg C. Applying the National Lung Screening Trial eligibility criteria to the US population: what percent of the population and of incident lung cancers would be covered. J Med Screen 2012; 19:154–156; with permission.)
References
-
- Pisano ED, Gatsonis G, Hendrick E, et al. Diagnostic performance of digital versus film mammography for breast-cancer screening. New Engl J Med. 2005;353:1773–1783. - PubMed
-
- Buys SS, Partridge E, Black A, et al. Effect of screening on ovarian cancer mortality: The Prostate, Lung, Colorectal and Ovarian (PLCO) cancer screening randomized controlled trial. J Amer Med Assoc. 2011;305:2295–2302. - PubMed
-
- Whitlock EP, Lin JS, Liles E, et al. Screening for colorectal cancer: a targeted, updated systematic review for the U.S. Preventive Services Task Force. Ann Int Med. 2008;149:638–658. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
