

Seizures in an immunocompromised adolescent: a case report
- PMID: 26315723
- PMCID: PMC4552135
- DOI: 10.1186/s13256-015-0660-2
Seizures in an immunocompromised adolescent: a case report
Abstract
Introduction: Tuberculosis is a progressive and disabling infection predominantly seen in low-income and middle-income countries. Immunocompromised patients are at a higher risk of contracting tuberculosis than the healthy population. The presentation may also be atypical, leading to delay in diagnosis. We report the first case of tuberculous cerebral vasculitis presenting with epilepsia partialis continua.
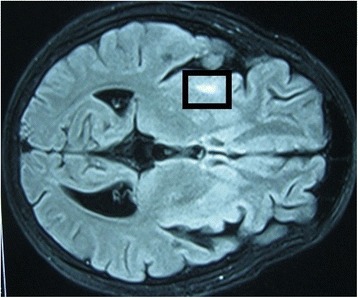
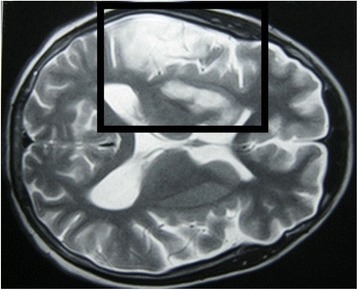
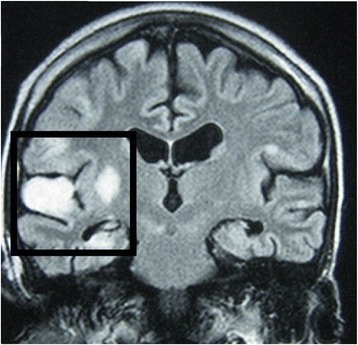
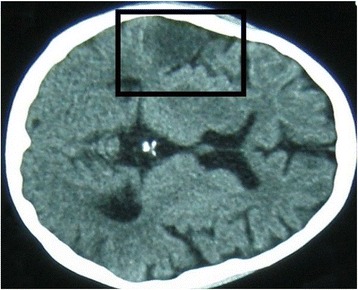
Case presentation: A 17-year-old adolescent boy of Sri Lankan Moor heritage was taking long-term immunosuppressants for nephrotic syndrome. He presented to hospital with focal fits affecting his left arm. He later developed choreiform movements of the same arm, progressing to epilepsia partialis continua and weakness. The gradually evolving focal neurological signs and underlying immunosuppression raised the possibility of localized cerebral infection or inflammation. Analysis of his cerebrospinal fluid showed lymphocytosis with normal cellular morphology. Magnetic resonance imaging was suggestive of progressive vasculitic infarctions of the cerebral cortex and basal ganglia. There was no evidence of active autoimmune or viral disease on hematological investigations, but molecular amplification detected Mycobacterium tuberculosis in his cerebrospinal fluid. Although our patient had been established on isoniazid preventive treatment for eight months before the episode, tuberculosis was nonetheless considered to be the most likely cause of the cerebral vasculitis. He was treated with a trial of anti-tuberculosis treatment, including streptomycin and adjunctive steroids, and made an uneventful recovery.
Conclusion: Clinicians should have a high index of suspicion for tuberculosis infection in patients with compromised immunity and other risk factors. The pathophysiological mechanisms underpinning cerebral vasculitis and epilepsia partialis continua are not completely understood. The efficacy of isoniazid prophylaxis in patients with immune suppression warrants further study. We present a regimen that successfully treated tuberculous cerebral vasculitis.
Figures
References
-
- Yoanna R, De Armasemail Y, Virginia C, Gustavo W, Luciano G, De Waard J. Sudden death related to tuberculous coronary arteritis. Int J Cardiol. 2011;156:e28–9. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
