

What accounts for ethnic differences in newborn skinfold thickness comparing South Asians and White Caucasians? Findings from the START and FAMILY Birth Cohorts
- PMID: 26315840
- PMCID: PMC4753357
- DOI: 10.1038/ijo.2015.171
What accounts for ethnic differences in newborn skinfold thickness comparing South Asians and White Caucasians? Findings from the START and FAMILY Birth Cohorts
Abstract
Objective: South Asians are a high-risk group for type 2 diabetes and coronary heart disease. We sought to determine ethnic differences in newborn adiposity comparing South Asians (SA) to White Caucasians (Whites).
Methods: Seven hundred ninety pregnant women (401 SA, 389 Whites) and their full-term offspring from two birth cohorts in Canada were analyzed. Pregnant women completed a health assessment including a 75-g oral glucose tolerance test to assess for dysglycemia. Birthweight, length, waist and hip circumference, and triceps and subscapular skinfold thickness (a surrogate measure of body adiposity) were measured in all newborns. Multivariate regression was used to identify maternal factors associated with newborn skinfold measurements.
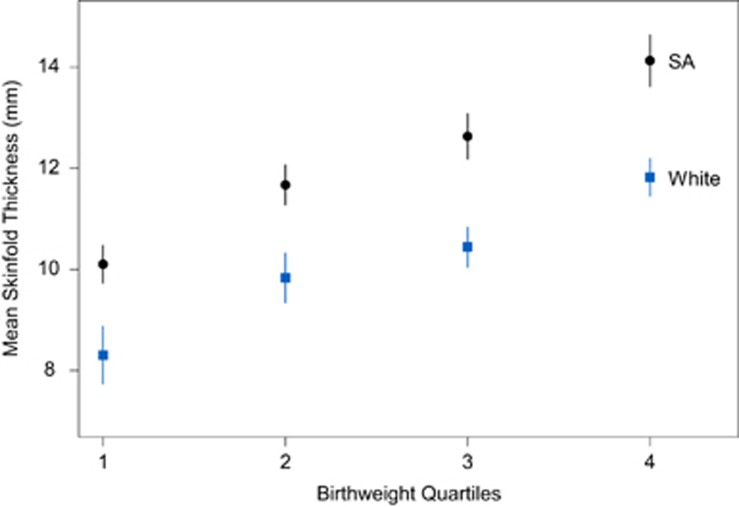
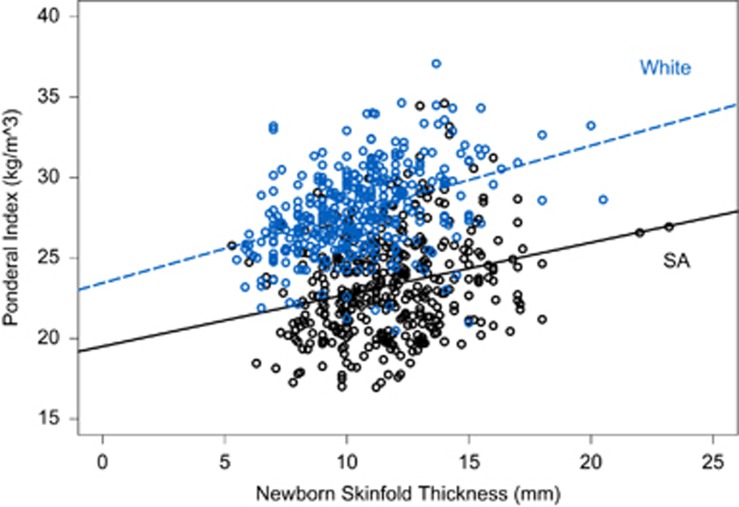
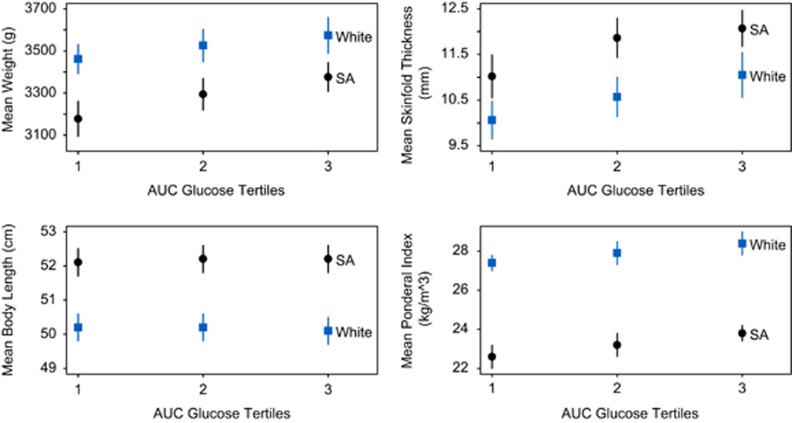
Results: South Asian women were younger (30.1 vs 31.8 years, P<0.001), their prepregnancy body mass index was lower (23.7 vs 26.2, P<0.0001) and gestational diabetes was substantially higher (21% vs 13%, P=0.005) compared with Whites. Among full-term newborns, South Asians had lower birthweight (3283 vs 3517 g, P=0.0001), had greater skinfold thickness (11.7 vs 10.6 mm; P=0.0001) and higher waist circumference (31.1 vs 29.9 cm, P=0.0001) compared with Whites. Risk factors for newborn skinfold thickness included South Asian ethnicity (standardized estimate (s.e.): 0.24; P<0.0001), maternal glucose (s.e.: 0.079; P=0.04) and maternal body fat (s.e.: 0.14; P=0.0002).
Conclusions: South Asian newborns are lower birthweight and have greater skinfold thickness, compared with White newborns, and this is influenced by maternal body fat and glucose. Interventions aimed at reducing body fat prior to pregnancy and gestational diabetes during pregnancy in South Asians may favorably alter newborn body composition and require evaluation.
Figures
References
-
- 1Anand SS, Yusuf S, Vuksan V, Devanesen S, Montague P, Kelemen L et al. Differences in risk factors, atherosclerosis, and cardiovascular disease between ethnic groups in Canada: the Study of Health Assessment and Risk in Ethnic Groups (SHARE). Lancet 2000; 356: 279–284. - PubMed
-
- 2Abate N, Chandalia M. Ethnicity and type 2 diabetes: focus on Asian Indians. J Diabetes Complications 2001; 15: 320–327. - PubMed
-
- 3Yajnik C, Fall C, Coyaji K, Hirve SS, Rao S, Barker DJ et al. Neonatal anthropometry: the thin-fat Indian baby. The Pune Maternal Nutrition Study. Ind J Obes Relat Metabol Disord 2003; 27: 173–180. - PubMed
-
- 4West J, Lawlor DA, Fairley L, Bhopal R, Cameron N, McKinney PA et al. UK-born Pakistani-origin infants are relatively more adipose than white British infants: findings from 8704 mother-offspring pairs in the Born-in-Bradford prospective birth cohort. J Epidemiol Community Health. 2013; 67: 544–551. - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
