

Efficient national surveillance for health-care-associated infections
- PMID: 26316148
- PMCID: PMC4552460
- DOI: 10.1186/s12889-015-2172-9
Efficient national surveillance for health-care-associated infections
Abstract
Background: Detecting novel healthcare-associated infections (HCAI) as early as possible is an important public health priority. However, there is currently no evidence base to guide the design of efficient and reliable surveillance systems. Here we address this issue in the context of a novel pathogen spreading primarily between hospitals through the movement of patients.
Methods: Using a mathematical modelling approach we compare the current surveillance system for a HCAI that spreads primarily between hospitals due to patient movements as it is implemented in Scotland with a gold standard to determine if the current system is maximally efficient or whether it would be beneficial to alter the number and choice of hospitals in which to concentrate surveillance effort.
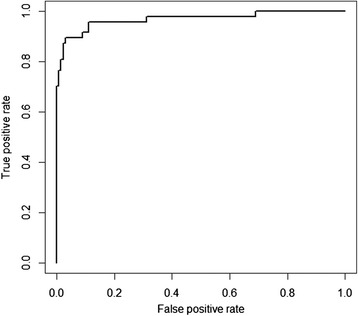
Results: We validated our model by demonstrating that it accurately predicts the risk of meticillin-resistant Staphylococcus aureus bacteraemia cases in Scotland. Using the 29 (out of 182) sentinel hospitals that currently contribute most of the national surveillance effort results in an average detection time of 117 days. A reduction in detection time to 87 days is possible by optimal selection of 29 hospitals. Alternatively, the same detection time (117 days) can be achieved using just 22 optimally selected hospitals. Increasing the number of sentinel hospitals to 38 (teaching and general hospitals) reduces detection time by 43 days; however decreasing the number to seven sentinel hospitals (teaching hospitals) increases detection time substantially to 268 days.
Conclusions: Our results show that the current surveillance system as it is used in Scotland is not optimal in detecting novel pathogens when compared to a gold standard. However, efficiency gains are possible by better choice of sentinel hospitals, or by increasing the number of hospitals involved in surveillance. Similar studies could be used elsewhere to inform the design and implementation of efficient national, hospital-based surveillance systems that achieve rapid detection of novel HCAIs for minimal effort.
Figures



References
-
- Stein RA. Antibiotic Resistance: A Global, Interdisciplinary Concern. Am Biol Teach. 2011;73(6):314–321. doi: 10.1525/abt.2011.73.6.3. - DOI
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
