

Systemic Atherosclerotic Inflammation Following Acute Myocardial Infarction: Myocardial Infarction Begets Myocardial Infarction
- PMID: 26316523
- PMCID: PMC4599491
- DOI: 10.1161/JAHA.115.001956
Systemic Atherosclerotic Inflammation Following Acute Myocardial Infarction: Myocardial Infarction Begets Myocardial Infarction
Abstract
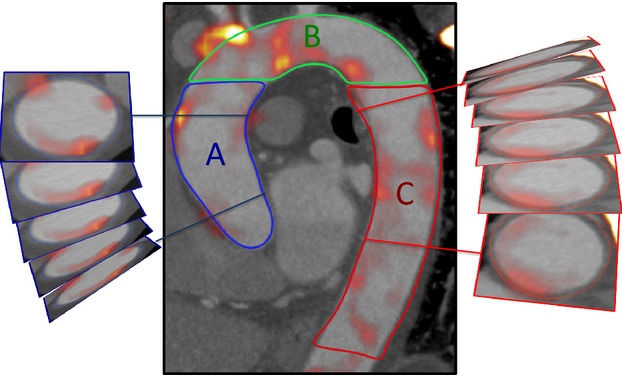
Background: Preclinical data suggest that an acute inflammatory response following myocardial infarction (MI) accelerates systemic atherosclerosis. Using combined positron emission and computed tomography, we investigated whether this phenomenon occurs in humans.
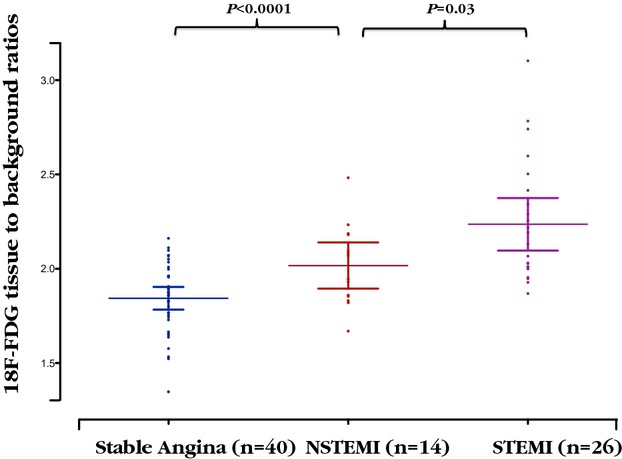
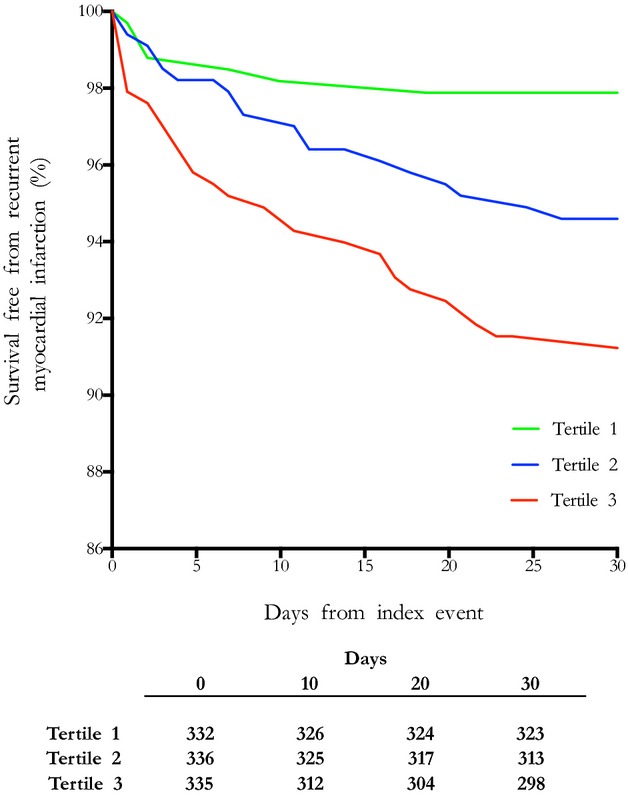
Methods and results: Overall, 40 patients with MI and 40 with stable angina underwent thoracic 18F-fluorodeoxyglucose combined positron emission and computed tomography scan. Radiotracer uptake was measured in aortic atheroma and nonvascular tissue (paraspinal muscle). In 1003 patients enrolled in the Global Registry of Acute Coronary Events, we assessed whether infarct size predicted early (≤30 days) and late (>30 days) recurrent coronary events. Compared with patients with stable angina, patients with MI had higher aortic 18F-fluorodeoxyglucose uptake (tissue-to-background ratio 2.15±0.30 versus 1.84±0.18, P<0.0001) and plasma C-reactive protein concentrations (6.50 [2.00 to 12.75] versus 2.00 [0.50 to 4.00] mg/dL, P=0.0005) despite having similar aortic (P=0.12) and less coronary (P=0.006) atherosclerotic burden and similar paraspinal muscular 18F-fluorodeoxyglucose uptake (P=0.52). Patients with ST-segment elevation MI had larger infarcts (peak plasma troponin 32 300 [10 200 to >50 000] versus 3800 [1000 to 9200] ng/L, P<0.0001) and greater aortic 18F-fluorodeoxyglucose uptake (2.24±0.32 versus 2.02±0.21, P=0.03) than those with non-ST-segment elevation MI. Peak plasma troponin concentrations correlated with aortic 18F-fluorodeoxyglucose uptake (r=0.43, P=0.01) and, on multivariate analysis, independently predicted early (tertile 3 versus tertile 1: relative risk 4.40 [95% CI 1.90 to 10.19], P=0.001), but not late, recurrent MI.
Conclusions: The presence and extent of MI is associated with increased aortic atherosclerotic inflammation and early recurrent MI. This finding supports the hypothesis that acute MI exacerbates systemic atherosclerotic inflammation and remote plaque destabilization: MI begets MI.
Clinical trial registration: URL: https://www.clinicaltrials.gov. Unique identifier: NCT01749254.
Keywords: 18F‐fluorodeoxyglucose positron emission and computed tomography; atherosclerosis; inflammation; vulnerable plaque.
© 2015 The Authors. Published on behalf of the American Heart Association, Inc., by Wiley Blackwell.
Figures
References
-
- Roger VL, Go AS, Lloyd-Jones DM, Adams RJ, Berry JD, Brown TM, Carnethon MR, Dai S, de Simone G, Ford ES, Fox CS, Fullerton HJ, Gillespie C, Greenlund KJ, Hailpern SM, Heit JA, Ho PM, Howard VJ, Kissela BM, Kittner SJ, Lackland DT, Lichtman JH, Lisabeth LD, Makuc DM, Marcus GM, Marelli A, Matchar DB, McDermott MM, Meigs JB, Moy CS, Mozaffarian D, Mussolino ME, Nichol G, Paynter NP, Rosamond WD, Sorlie PD, Stafford RS, Turan TN, Turner MB, Wong ND, Wylie-Rosett J. Heart disease and stroke statistics—2011 update: a report from the American Heart Association. Circulation. 2011;123:e18–e209. - PMC - PubMed
-
- Naghavi M, Libby P, Falk E, Casscells SW, Litovsky S, Rumberger J, Badimon JJ, Stefanadis C, Moreno P, Pasterkamp G, Fayad Z, Stone PH, Waxman S, Raggi P, Madjid M, Zarrabi A, Burke A, Yuan C, Fitzgerald PJ, Siscovick DS, de Korte CL, Aikawa M, Juhani Airaksinen KE, Assmann G, Becker CR, Chesebro JH, Farb A, Galis ZS, Jackson C, Jang IK, Koenig W, Lodder RA, March K, Demirovic J, Navab M, Priori SG, Rekhter MD, Bahr R, Grundy SM, Mehran R, Colombo A, Boerwinkle E, Ballantyne C, Insull W, Jr, Schwartz RS, Vogel R, Serruys PW, Hansson GK, Faxon DP, Kaul S, Drexler H, Greenland P, Muller JE, Virmani R, Ridker PM, Zipes DP, Shah PK, Willerson JT. From vulnerable plaque to vulnerable patient: a call for new definitions and risk assessment strategies: part I. Circulation. 2003;108:1664–1672. - PubMed
-
- Virmani R, Kolodgie FD, Burke AP, Farb A, Schwartz SM. Lessons from sudden coronary death: a comprehensive morphological classification scheme for atherosclerotic lesions. Arterioscler Thromb Vasc Biol. 2000;20:1262–1275. - PubMed
-
- Milonas C, Jernberg T, Lindback J, Agewall S, Wallentin L, Stenestrand U. Effect of angiotensin-converting enzyme inhibition on one-year mortality and frequency of repeat acute myocardial infarction in patients with acute myocardial infarction. Am J Cardiol. 2010;105:1229–1234. - PubMed
-
- Goldstein JA, Demetriou D, Grines CL, Pica M, Shoukfeh M, O’Neill WW. Multiple complex coronary plaques in patients with acute myocardial infarction. N Engl J Med. 2000;343:915–922. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
- PG/09/083/27667/BHF_/British Heart Foundation/United Kingdom
- FS/10/024/28266/BHF_/British Heart Foundation/United Kingdom
- FS/12/83/29781/BHF_/British Heart Foundation/United Kingdom
- FS/12/84/29814/BHF_/British Heart Foundation/United Kingdom
- WT103782AIA/WT_/Wellcome Trust/United Kingdom
- 103782/WT_/Wellcome Trust/United Kingdom
- PG/12/8/BHF_/British Heart Foundation/United Kingdom
- FS/14/78/31020/BHF_/British Heart Foundation/United Kingdom
- FS/12/29/29463/BHF_/British Heart Foundation/United Kingdom
- G0701127/MRC_/Medical Research Council/United Kingdom
- ETM/160/CSO_/Chief Scientist Office/United Kingdom
- PG/12/8/29371/BHF_/British Heart Foundation/United Kingdom
- FS/10/026/BHF_/British Heart Foundation/United Kingdom
- CH/09/002/BHF_/British Heart Foundation/United Kingdom
- FS/10/024/BHF_/British Heart Foundation/United Kingdom
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
