

Intracellular Na+ Concentration ([Na+]i) Is Elevated in Diabetic Hearts Due to Enhanced Na+-Glucose Cotransport
- PMID: 26316524
- PMCID: PMC4599504
- DOI: 10.1161/JAHA.115.002183
Intracellular Na+ Concentration ([Na+]i) Is Elevated in Diabetic Hearts Due to Enhanced Na+-Glucose Cotransport
Abstract
Background: Intracellular Na(+) concentration ([Na(+)]i) regulates Ca(2+) cycling, contractility, metabolism, and electrical stability of the heart. [Na(+)]i is elevated in heart failure, leading to arrhythmias and oxidative stress. We hypothesized that myocyte [Na(+)]i is also increased in type 2 diabetes (T2D) due to enhanced activity of the Na(+)-glucose cotransporter.
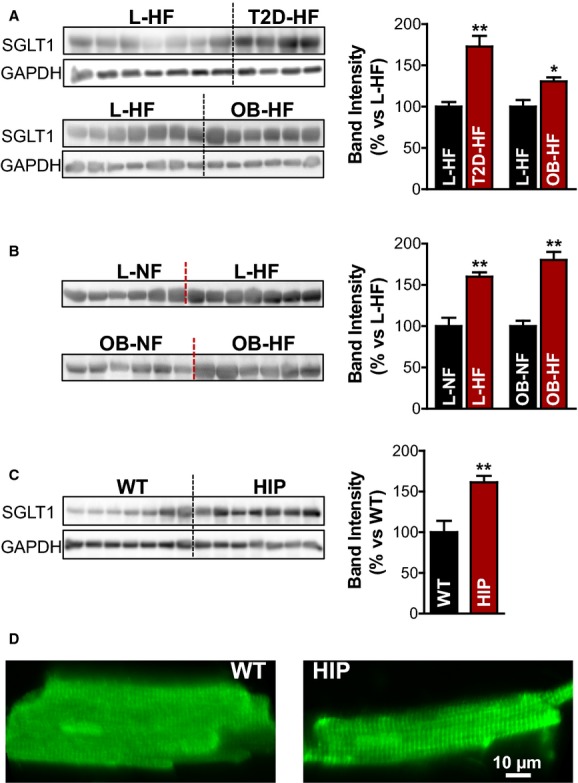
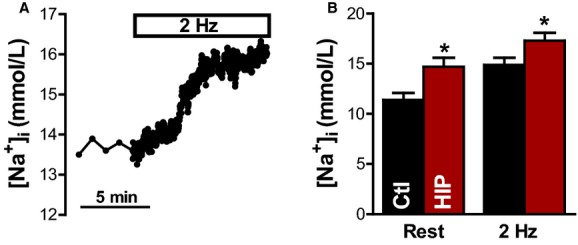
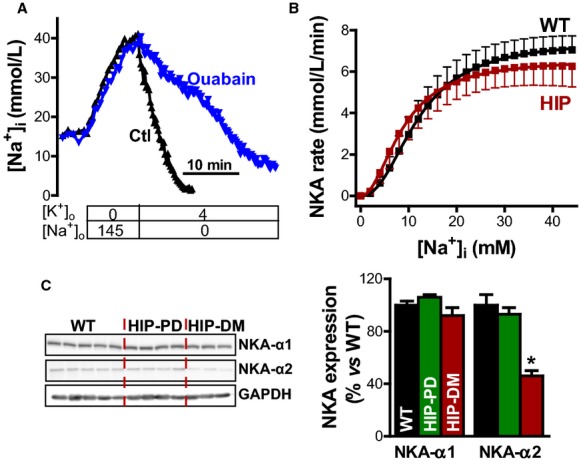
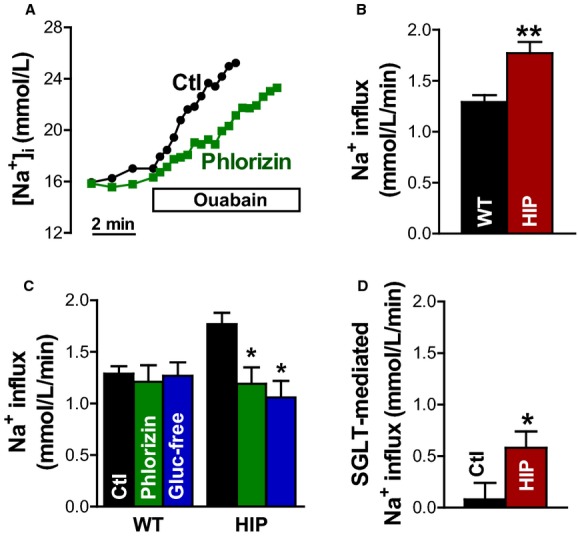
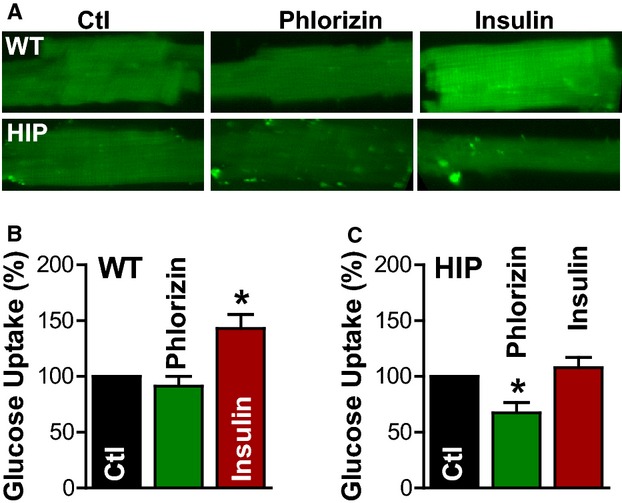
Methods and results: To test this hypothesis, we used myocardial tissue from humans with T2D and a rat model of late-onset T2D (HIP rat). Western blot analysis showed increased Na(+)-glucose cotransporter expression in failing hearts from T2D patients compared with nondiabetic persons (by 73±13%) and in HIP rat hearts versus wild-type (WT) littermates (by 61±8%). [Na(+)]i was elevated in HIP rat myocytes both at rest (14.7±0.9 versus 11.4±0.7 mmol/L in WT) and during electrical stimulation (17.3±0.8 versus 15.0±0.7 mmol/L); however, the Na(+)/K(+)-pump function was similar in HIP and WT cells, suggesting that higher [Na(+)]i is due to enhanced Na(+) entry in diabetic hearts. Indeed, Na(+) influx was significantly larger in myocytes from HIP versus WT rats (1.77±0.11 versus 1.29±0.06 mmol/L per minute). Na(+)-glucose cotransporter inhibition with phlorizin or glucose-free solution greatly reduced Na(+) influx in HIP myocytes (to 1.20±0.16 mmol/L per minute), whereas it had no effect in WT cells. Phlorizin also significantly decreased glucose uptake in HIP myocytes (by 33±9%) but not in WT, indicating an increased reliance on the Na(+)-glucose cotransporter for glucose uptake in T2D hearts.
Conclusions: Myocyte Na(+)-glucose cotransport is enhanced in T2D, which increases Na(+) influx and causes Na(+) overload. Higher [Na(+)]i may contribute to arrhythmogenesis and oxidative stress in diabetic hearts.
Keywords: Na+–glucose cotransporter; heart; intracellular Na+ concentration; type 2 diabetes.
© 2015 The Authors. Published on behalf of the American Heart Association, Inc., by Wiley Blackwell.
Figures
References
-
- Devereux RB, Roman MJ, Paranicas M, O’Grady MJ, Lee ET, Welty TK, Fabsitz RR, Robbins D, Rhoades ER, Howard BV. Impact of diabetes on cardiac structure and function: the Strong Heart Study. Circulation. 2000;101:2271–2276. - PubMed
-
- Taegtmeyer H, McNulty P, Young ME. Adaptation and maladaptation of the heart in diabetes: part I: general concepts. Circulation. 2002;105:1727–1733. - PubMed
-
- Young LH, Wackers FJ, Chyun DA, Davey JA, Barrett EJ, Taillefer R, Heller GV, Iskandrian AE, Wittlin SD, Filipchuk N, Ratner RE, Inzucchi SE DIAD Investigators. Cardiac outcomes after screening for asymptomatic coronary artery disease in patients with type 2 diabetes: the DIAD study: a randomized controlled trial. JAMA. 2009;301:1547–1555. - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
