

Sex-Specific Association of Sleep Apnea Severity With Subclinical Myocardial Injury, Ventricular Hypertrophy, and Heart Failure Risk in a Community-Dwelling Cohort: The Atherosclerosis Risk in Communities-Sleep Heart Health Study
- PMID: 26316620
- PMCID: PMC4596785
- DOI: 10.1161/CIRCULATIONAHA.115.016985
Sex-Specific Association of Sleep Apnea Severity With Subclinical Myocardial Injury, Ventricular Hypertrophy, and Heart Failure Risk in a Community-Dwelling Cohort: The Atherosclerosis Risk in Communities-Sleep Heart Health Study
Abstract
Background: Risk factors for obstructive sleep apnea (OSA) and the development of subsequent cardiovascular (CV) complications differ by sex. We hypothesize that the relationship between OSA and high-sensitivity troponin T (hs-TnT), cardiac structure, and CV outcomes differs by sex.
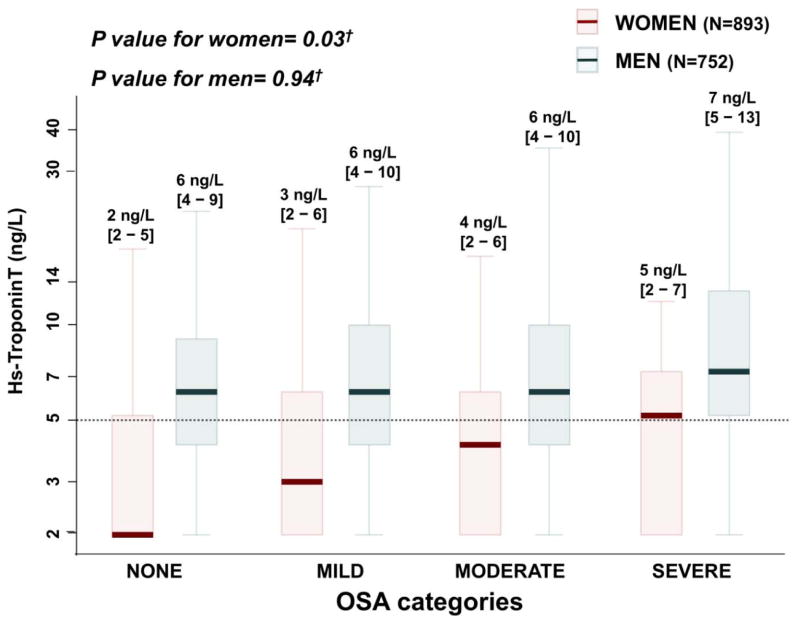
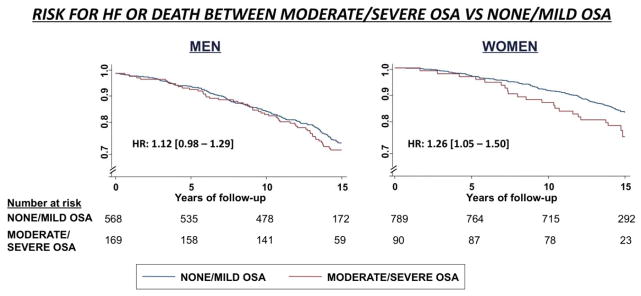
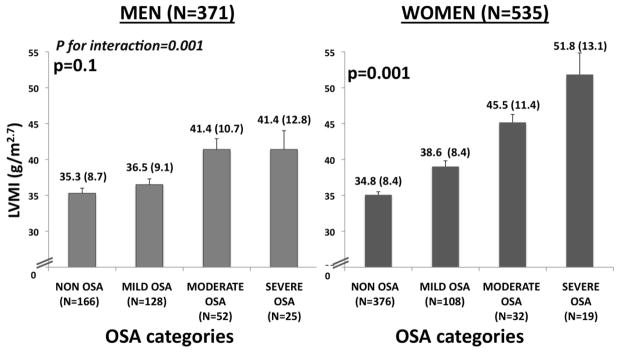
Methods and results: Seven hundred fifty-two men and 893 women free of CV disease participating in both the Atherosclerosis Risk in the Communities and the Sleep Heart Health Studies were included. All participants (mean age, 62.5 ± 5.5 years) underwent polysomnography and measurement of hs-TnT. OSA severity was defined by using established clinical categories. Subjects were followed for 13.6 ± 3.2 years for incident coronary disease, heart failure, and CV and all-cause mortality. Surviving subjects underwent echocardiography after 15.2 ± 0.8 years. OSA was independently associated with hs-TnT among women (P=0.03) but not in men (P=0.94). Similarly, OSA was associated with incident heart failure or death in women (P=0.01) but not men (P=0.10). This association was no longer significant after adjusting for hs-TnT (P=0.09). Among surviving participants without an incident CV event, OSA assessed in midlife was independently associated with higher left ventricle mass index only among women (P=0.001).
Conclusions: Sex-specific differences exist in the relationship between OSA and CV disease. OSA, assessed in midlife, is independently associated with higher levels of concomitantly measured hs-TnT among women but not men, in whom other comorbidities associated with OSA may play a more important role. During 13-year follow-up, OSA was associated with incident heart failure or death only among women, and, among those without an incident event, it was independently associated with left ventricular hypertrophy only in women.
Keywords: echocardiography; heart failure; sex; sleep disorders; troponin T.
© 2015 American Heart Association, Inc.
Figures
Comment in
-
Risk of Obstructive Sleep Apnea: Sex Matters.Circulation. 2015 Oct 6;132(14):1305-6. doi: 10.1161/CIRCULATIONAHA.115.018694. Epub 2015 Aug 27. Circulation. 2015. PMID: 26316619 No abstract available.
References
-
- Young T, Palta M, Dempsey J, Skatrud J, Weber S, Badr S. The occurrence of sleep-disordered breathing among middle-aged adults. N Engl J Med. 1993;328:1230–1235. - PubMed
-
- Young T, Peppard PE, Gottlieb DJ. Epidemiology of obstructive sleep apnea. Am J Respir Crit Care Med. 2002;165:1217–1239. - PubMed
-
- Quintana-Gallego E, Carmon-Bernal C, Capote F, Sánchez-Armengol A, Botebol-Benhamou G, Polo-Padillo, Castillo-Gomez J. Gender differences in obstructive sleep apnea syndrome: a clinical study of 1166 patients. Respir Med. 2004;98:984–9. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- HHSN268201100012C/HL/NHLBI NIH HHS/United States
- K08 HL116792/HL/NHLBI NIH HHS/United States
- HHSN268201100009I/HL/NHLBI NIH HHS/United States
- 268201100011C/PHS HHS/United States
- 268201100005C/PHS HHS/United States
- HHSN268201100010C/HL/NHLBI NIH HHS/United States
- 268201100007C/PHS HHS/United States
- HHSN268201100008C/HL/NHLBI NIH HHS/United States
- U01 HL063463/HL/NHLBI NIH HHS/United States
- HHSN268201100005G/HL/NHLBI NIH HHS/United States
- HHSN268201100008I/HL/NHLBI NIH HHS/United States
- HC-11-08/HC/NHLBI NIH HHS/United States
- HHSN268201100007C/HL/NHLBI NIH HHS/United States
- 268201100012C/PHS HHS/United States
- 268201100008C/PHS HHS/United States
- HHSN268201100011I/HL/NHLBI NIH HHS/United States
- HHSN268201100011C/HL/NHLBI NIH HHS/United States
- U01HL53934/HL/NHLBI NIH HHS/United States
- HHSN268201100006C/HL/NHLBI NIH HHS/United States
- 268 201100009C/PHS HHS/United States
- HHSN268201100005I/HL/NHLBI NIH HHS/United States
- U01 HL053934/HL/NHLBI NIH HHS/United States
- HHSN268201100009C/HL/NHLBI NIH HHS/United States
- HHSN268201100005C/HL/NHLBI NIH HHS/United States
- 268201100006C/PHS HHS/United States
- 268201100010C/PHS HHS/United States
- HHSN268201100007I/HL/NHLBI NIH HHS/United States
- K08-HL-116792/HL/NHLBI NIH HHS/United States
- U01HL53940/HL/NHLBI NIH HHS/United States
- U01HL63463/HL/NHLBI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Medical
