

Reduction of exercise capacity in sarcoidosis in relation to disease severity
- PMID: 26316723
- PMCID: PMC4547650
- DOI: 10.2147/PPA.S86465
Reduction of exercise capacity in sarcoidosis in relation to disease severity
Abstract
Introduction: Pulmonary function tests (PFTs) do not always predict functional limitations during exercise in sarcoidosis. Cardiopulmonary exercise testing (CPET) may facilitate the recognition of exercise intolerance in these patients.
Aim: As relevant data in sarcoid patients are limited, the aim of the study reported here was to assess exercise capacity impairment during a maximal CPET and to evaluate potential correlations with PFT measurements and radiological stages of the disease.
Method: A total of 83 sarcoid patients consecutively referred for evaluation of exertional dyspnea over a 3-year period were studied retrospectively with PFTs, including spirometry, diffusing capacity of the lung for carbon monoxide (DLCO) and lung volumes, and CPET using standard protocol. Patients were grouped according to their radiological stages: Stage I (n=43), Stages II-III (n=31), and Stage IV (n=9).
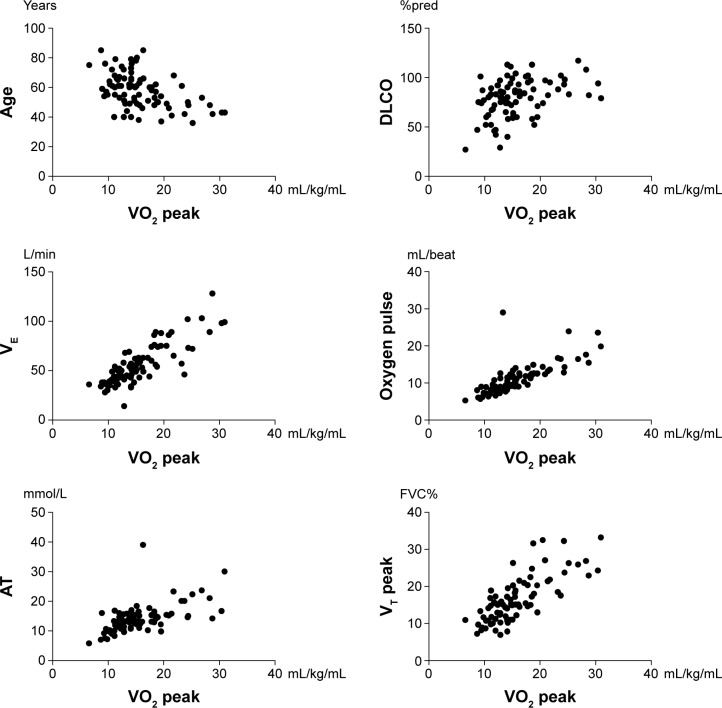
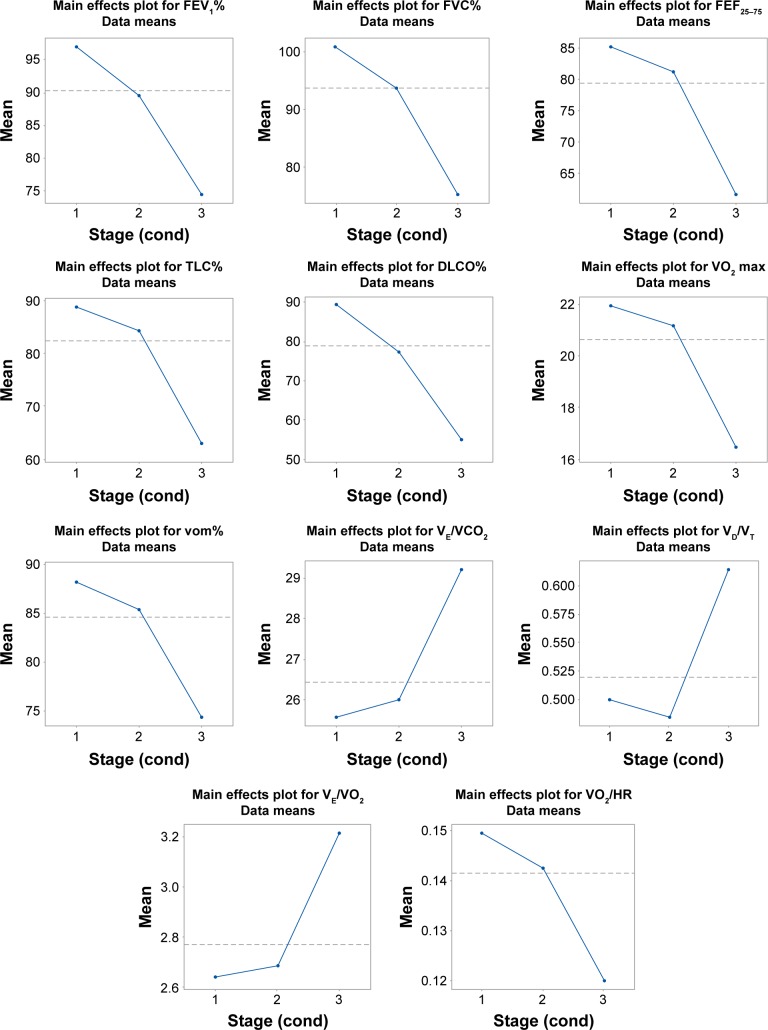
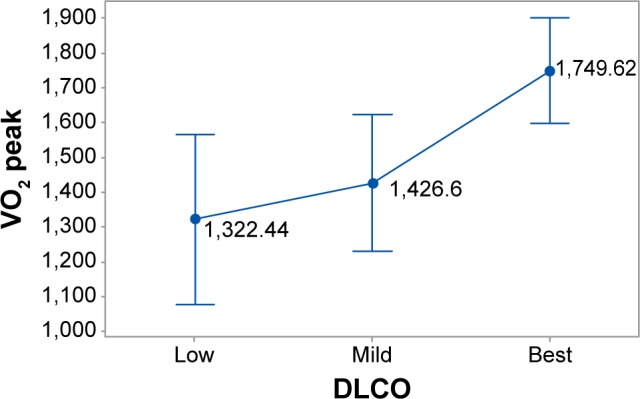
Results: Forced expiratory volume in 1 second, forced vital capacity, and total lung capacity were mildly impaired only in Stage IV (means ± standard deviation: 72.44±28.00, 71.33±26.70, and 59.78±21.72, respectively), while DLCO was mildly and moderately reduced in Stages II-III and IV (72.68±14.13 and 51.22±18.50, respectively) and differed significantly between all stages (I vs II-III: P=0.003, I vs IV: P=0.003, and II-III vs IV: P=0.009). Exercise capacity (as expressed by peak oxygen consumption <84% predicted) was decreased in 53% of patients (Stage I: 48%, Stages II-III: 52%, Stage IV: 78%); however, significant differences were noticed only between Stages I and IV (P=0.0025). Of note, significant correlations were found between peak oxygen consumption and DLCO (P=0.0083), minute ventilation (P<0.0001), oxygen pulse (P<0.0001), lactate threshold (P<0.0001), and peak ventilatory threshold (P<0.0001).
Conclusion: CPET could be considered a useful tool in exercise intolerance evaluation in sarcoid patients with mild PFT abnormalities. Exercise limitation in sarcoidosis may be attributed to both ventilatory and cardiocirculatory impairment.
Keywords: cardiopulmonary exercise testing; exercise; pulmonary function tests.
Figures
Similar articles
-
Reduction of maximal oxygen uptake in sarcoidosis: relationship with disease severity.Respiration. 2011;82(6):501-8. doi: 10.1159/000330050. Epub 2011 Sep 20. Respiration. 2011. PMID: 21934275
-
Exercise capacity in sarcoidosis. Study of 29 patients.Med Clin (Barc). 2005 May 14;124(18):686-9. doi: 10.1157/13075090. Med Clin (Barc). 2005. PMID: 15899162
-
[Exercise capacity in patients with pulmonary sarcoidosis].Pol Merkur Lekarski. 2017 Aug 21;43(254):61-65. Pol Merkur Lekarski. 2017. PMID: 28875971 Polish.
-
Cardiopulmonary exercise testing in the functional and prognostic evaluation of patients with pulmonary diseases.Respiration. 2009;77(1):3-17. doi: 10.1159/000186694. Epub 2009 Jan 14. Respiration. 2009. PMID: 19145106 Review.
-
Cardiopulmonary Exercise Testing in Patients With Interstitial Lung Disease.Front Physiol. 2020 Jul 10;11:832. doi: 10.3389/fphys.2020.00832. eCollection 2020. Front Physiol. 2020. PMID: 32754054 Free PMC article. Review.
Cited by
-
Low-dose Naltrexone for the treatment of sarcoidosis.Sarcoidosis Vasc Diffuse Lung Dis. 2017;34(2):184-187. doi: 10.36141/svdld.v34i2.5303. Epub 2017 Apr 28. Sarcoidosis Vasc Diffuse Lung Dis. 2017. PMID: 32476841 Free PMC article.
-
Cardiopulmonary exercise testing in interstitial lung diseases and the value of ventilatory efficiency.Eur Respir Rev. 2021 Nov 30;30(162):200355. doi: 10.1183/16000617.0355-2020. Print 2021 Dec 31. Eur Respir Rev. 2021. PMID: 34853093 Free PMC article. Review.
-
Patient reported outcome measures (PROMs) in sarcoidosis.Sarcoidosis Vasc Diffuse Lung Dis. 2017;34(1):2-17. doi: 10.36141/svdld.v34i1.5760. Epub 2017 Apr 28. Sarcoidosis Vasc Diffuse Lung Dis. 2017. PMID: 32476819 Free PMC article. Review.
-
Spirometry, cardiopulmonary exercise testing and the six-minute walk test results in sarcoidosis patients.Sarcoidosis Vasc Diffuse Lung Dis. 2019;36(3):185-194. doi: 10.36141/svdld.v36i3.7663. Epub 2019 May 1. Sarcoidosis Vasc Diffuse Lung Dis. 2019. PMID: 32476953 Free PMC article.
-
Cardiopulmonary exercise testing complements both spirometry and nuclear imaging for assessing sarcoidosis stage and for monitoring disease activity.Sarcoidosis Vasc Diffuse Lung Dis. 2024 Mar 26;41(1):e2024017. doi: 10.36141/svdld.v41i1.15125. Sarcoidosis Vasc Diffuse Lung Dis. 2024. PMID: 38567559 Free PMC article.
References
-
- Statement on sarcoidosis Joint Statement of the American Thoracic Society (ATS), the European Respiratory Society (ERS) and the World Association of Sarcoidosis and Other Granulomatous Disorders (WASOG) adopted by the ATS Board of Directors and by the ERS Executive Committee, February 1999. Am J Respir Crit Care Med. 1999;160(2):736–755. - PubMed
-
- Drent M, Lower EE, De Vries J. Sarcoidosis-associated fatigue. Eur Respir J. 2012;40(1):255–263. - PubMed
-
- Marcellis RG, Lenssen AF, Elfferich MD, et al. Exercise capacity, muscle strength and fatigue in sarcoidosis. Eur Respir J. 2011;38(3):628–634. - PubMed
-
- Winterbauer RH, Hutchinson JF. Use of pulmonary function tests in the management of sarcoidosis. Chest. 1980;78(4):640–647. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
