

Controlling myopia progression in children and adolescents
- PMID: 26316834
- PMCID: PMC4542412
- DOI: 10.2147/AHMT.S55834
Controlling myopia progression in children and adolescents
Abstract
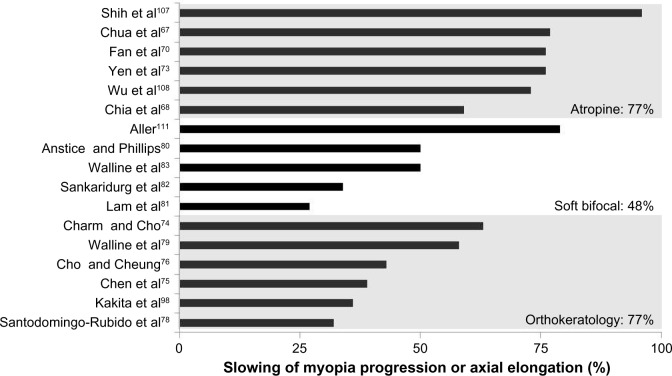
Myopia is a common disorder, affecting approximately one-third of the US population and over 90% of the population in some East Asian countries. High amounts of myopia are associated with an increased risk of sight-threatening problems, such as retinal detachment, choroidal degeneration, cataracts, and glaucoma. Slowing the progression of myopia could potentially benefit millions of children in the USA. To date, few strategies used for myopia control have proven to be effective. Treatment options such as undercorrection of myopia, gas permeable contact lenses, and bifocal or multifocal spectacles have all been proven to be ineffective for myopia control, although one recent randomized clinical trial using executive top bifocal spectacles on children with progressive myopia has shown to decrease the progression to nearly half of the control subjects. The most effective methods are the use of orthokeratology contact lenses, soft bifocal contact lenses, and topical pharmaceutical agents such as atropine or pirenzepine. Although none of these modalities are US Food and Drug Administration-approved to slow myopia progression, they have been shown to slow the progression by approximately 50% with few risks. Both orthokeratology and soft bifocal contact lenses have shown to slow myopia progression by slightly less than 50% in most studies. Parents and eye care practitioners should work together to determine which modality may be best suited for a particular child. Topical pharmaceutical agents such as anti-muscarinic eye drops typically lead to light sensitivity and poor near vision. The most effective myopia control is provided by atropine, but is rarely prescribed due to the side effects. Pirenzepine provides myopia control with little light sensitivity and few near-vision problems, but it is not yet commercially available as an eye drop or ointment. Several studies have shown that lower concentrations of atropine slow the progression of myopia control with fewer side effects than 1% atropine. While the progression of myopic refractive error is slowed with lower concentration of atropine, the growth of the eye is not, indicating a potentially reversible form of myopia control that may diminish after discontinuation of the eye drops. This review provides an overview of the myopia control information available in the literature and raises questions that remain unanswered, so that eye care practitioners and parents can potentially learn the methods that may ultimately improve a child's quality of life or lower the risk of sight-threatening complications.
Keywords: atropine; children; myopia control; orthokeratology; review; soft bifocal contact lenses.
Figures
References
-
- Garner LF, Owens H, Kinnear RF, Frith MJ. Prevalence of myopia in Sherpa and Tibetan children in Nepal. Optom Vis Sci. 1999;76(5):282–285. - PubMed
-
- Wang TJ, Chiang TH, Wang TH, Lin LL, Shih YF. Changes of the ocular refraction among freshmen in National Taiwan University between 1988 and 2005. Eye (Lond) 2009;23(5):1168–1169. - PubMed
-
- Ip JM, Huynh SC, Robaei D, et al. Ethnic differences in refraction and ocular biometry in a population-based sample of 11–15-year-old Australian children. Eye (Lond) 2008;22(5):649–656. - PubMed
-
- Ip JM, Huynh SC, Robaei D, et al. Ethnic differences in the impact of parental myopia: findings from a population-based study of 12-year-old Australian children. Invest Ophthalmol Vis Sci. 2007;48(6):2520–2528. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
