

The Sleeve Bypass Trial: a multicentre randomized controlled trial comparing the long term outcome of laparoscopic sleeve gastrectomy and gastric bypass for morbid obesity in terms of excess BMI loss percentage and quality of life
- PMID: 26316928
- PMCID: PMC4550059
- DOI: 10.1186/s40608-015-0058-0
The Sleeve Bypass Trial: a multicentre randomized controlled trial comparing the long term outcome of laparoscopic sleeve gastrectomy and gastric bypass for morbid obesity in terms of excess BMI loss percentage and quality of life
Abstract
Background: Obesity is an increasing disease worldwide. Bariatric surgery is the only effective therapy to induce sufficient long-term weight loss for morbidly obese patients. Laparoscopic Roux-en-Y Gastric Bypass (LRYGB) is the gold standard surgical technique. Laparoscopic Sleeve Gastrectomy (LSG) is a new promising bariatric procedure which has the advantage of maintaining an intact gastrointestinal tract. The aim of this study is to evaluate the efficiency of both techniques. Our hypothesis is that LSG has a similar percentage excess BMI loss (%EBMIL) after 5 years compared to LRYGB.
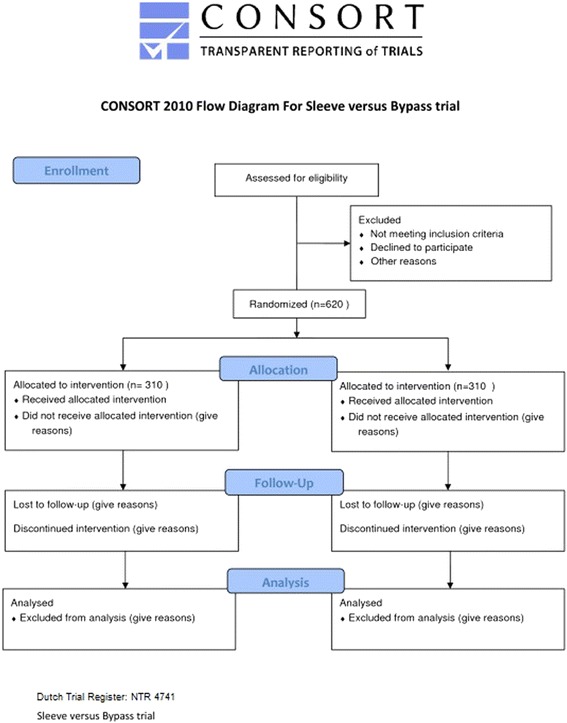
Methods/design: The Sleeve Bypass Trial is a randomized multicentre clinical trial: patients eligible for bariatric surgery are randomized to either LSG or LRYGB. Patients with a body mass index (BMI) ≥ 40 kg/m(2) or BMI 35 kg/m(2) with obesity related comorbidity (T2 DM, sleep apnoea, hypertension) are eligible for randomization. At randomization patients are stratified for centre, sex, T2 DM and BMI ≥ 50 kg/m(2). A total number of 620 patients will be enrolled and equally (1:1) randomized to both treatment arms. Only surgeons experienced in both operation techniques will participate in the Sleeve Bypass trial. The primary endpoint is the 5-year weight loss (%EBMIL) of LSG and LRYGB. Secondary endpoints are resolution of obesity related comorbidity, complications, revision bariatric surgery and quality of life (QOL) defined in various questionnaires.
Discussion: Long-term %EBMIL between the two treatment strategies used to be in favour of LRYGB, but more recent results throughout the world show similar %EBMIL in both techniques. If weight loss is comparable, obesity-related comorbidity and QOL after bariatric procedures should be taken into account when deciding on which surgical technique is to be preferred for certain subgroups in the future.
Trial registration: Dutch Trial Register: NTR 4741.
Keywords: Bariatric surgery; Bypass; Sleeve.
References
-
- James PT, Rigby N, Leach R; International Obesity Task Force. The obesity epidemic, metabolic syndrome and future prevention strategies. Eur J Carddiovasc Prev Rehab. 2004;11:3–8. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
