

Multimorbidity and Patient Safety Incidents in Primary Care: A Systematic Review and Meta-Analysis
- PMID: 26317435
- PMCID: PMC4552710
- DOI: 10.1371/journal.pone.0135947
Multimorbidity and Patient Safety Incidents in Primary Care: A Systematic Review and Meta-Analysis
Abstract
Background: Multimorbidity is increasingly prevalent and represents a major challenge in primary care. Patients with multimorbidity are potentially more likely to experience safety incidents due to the complexity of their needs and frequency of their interactions with health services. However, rigorous syntheses of the link between patient safety incidents and multimorbidity are not available. This review examined the relationship between multimorbidity and patient safety incidents in primary care.
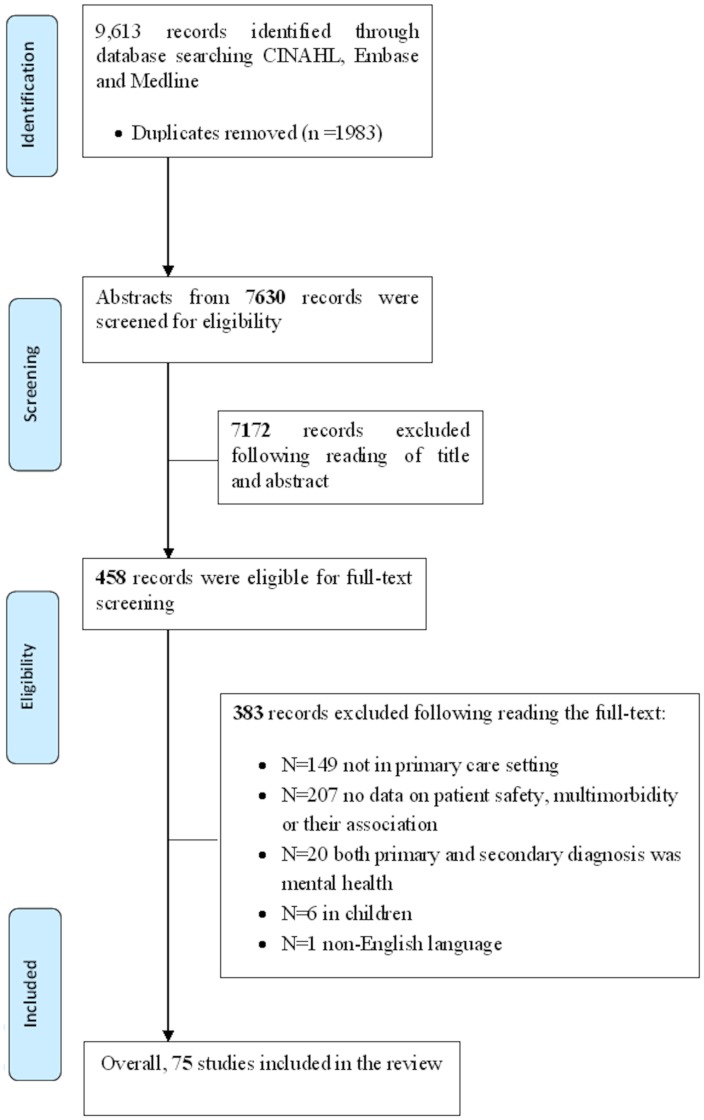
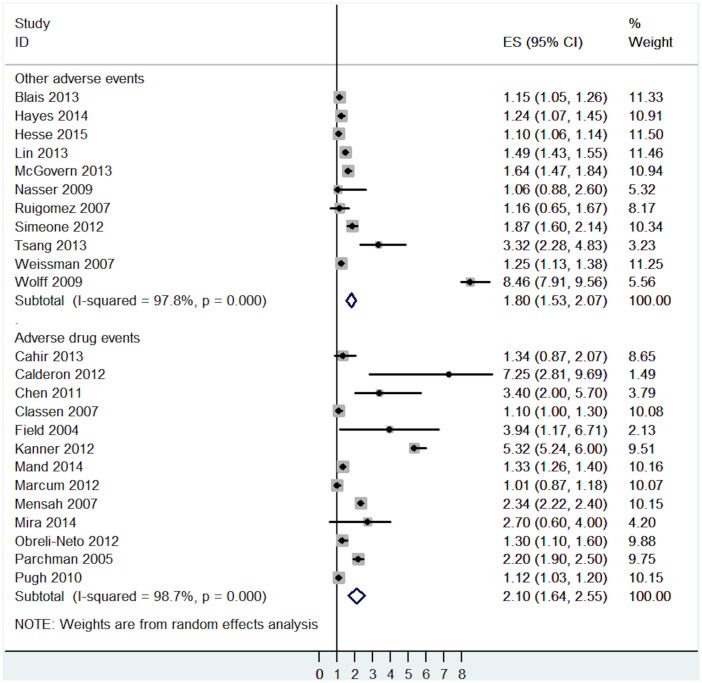
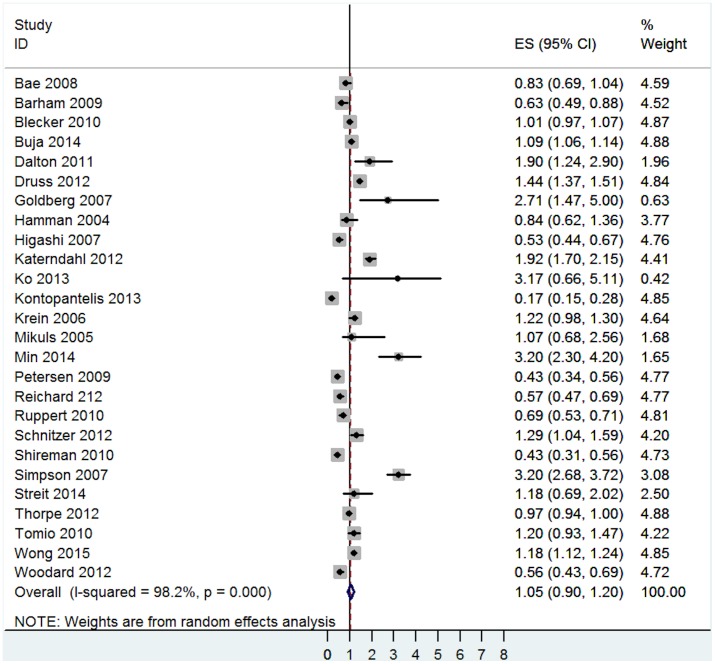
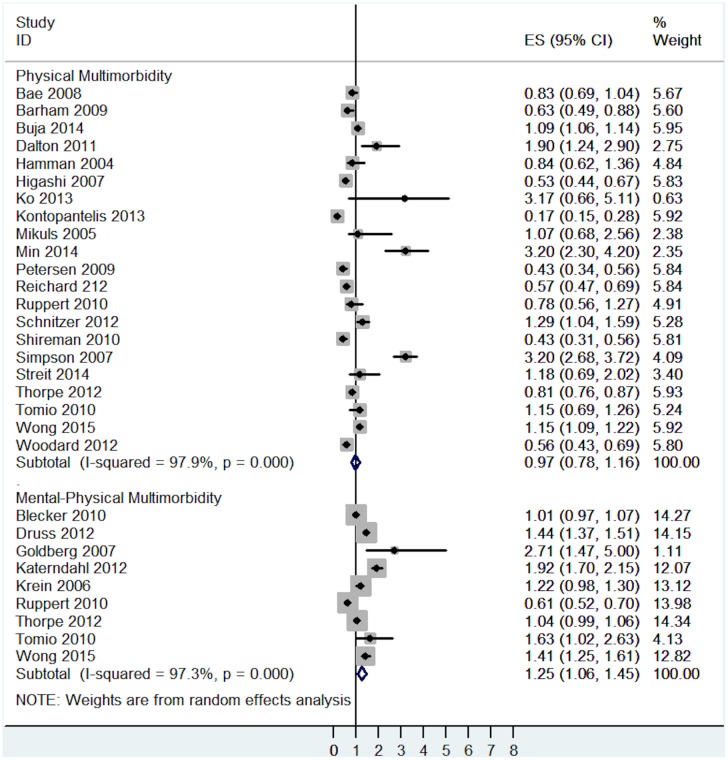
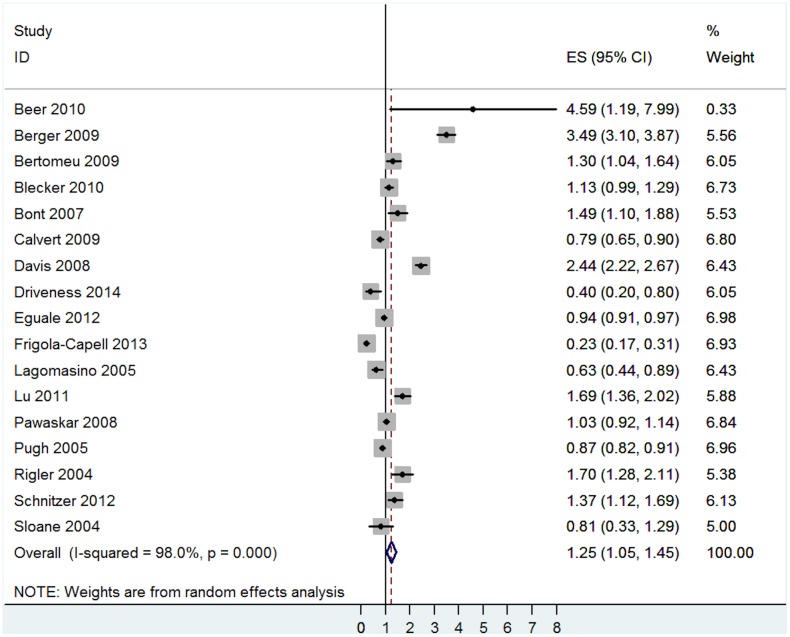
Methods: We followed our published protocol (PROSPERO registration number: CRD42014007434). Medline, Embase and CINAHL were searched up to May 2015. Study design and quality were assessed. Odds ratios (OR) and 95% confidence intervals (95% CIs) were calculated for the associations between multimorbidity and two categories of patient safety outcomes: 'active patient safety incidents' (such as adverse drug events and medical complications) and 'precursors of safety incidents' (such as prescription errors, medication non-adherence, poor quality of care and diagnostic errors). Meta-analyses using random effects models were undertaken.
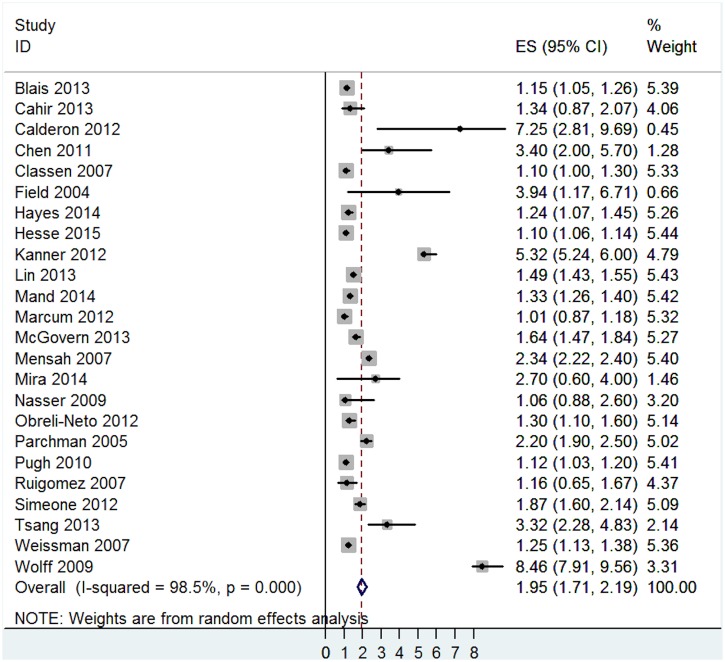
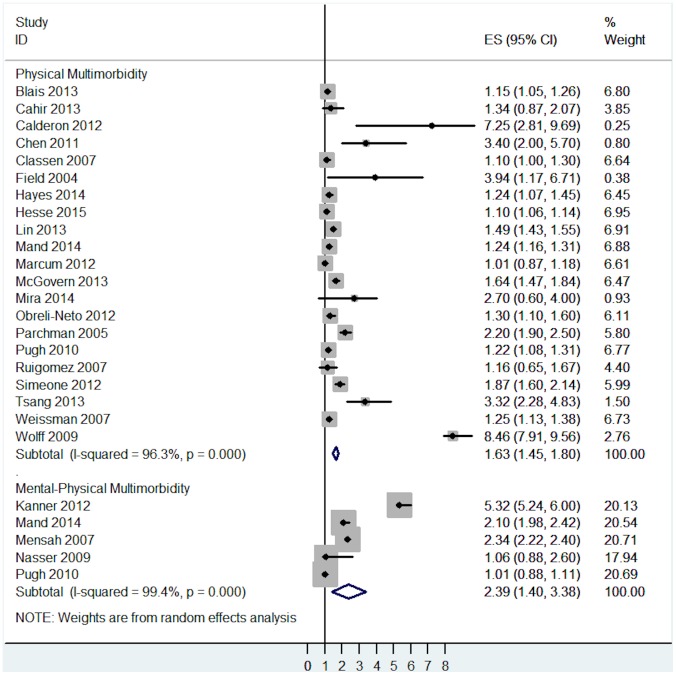
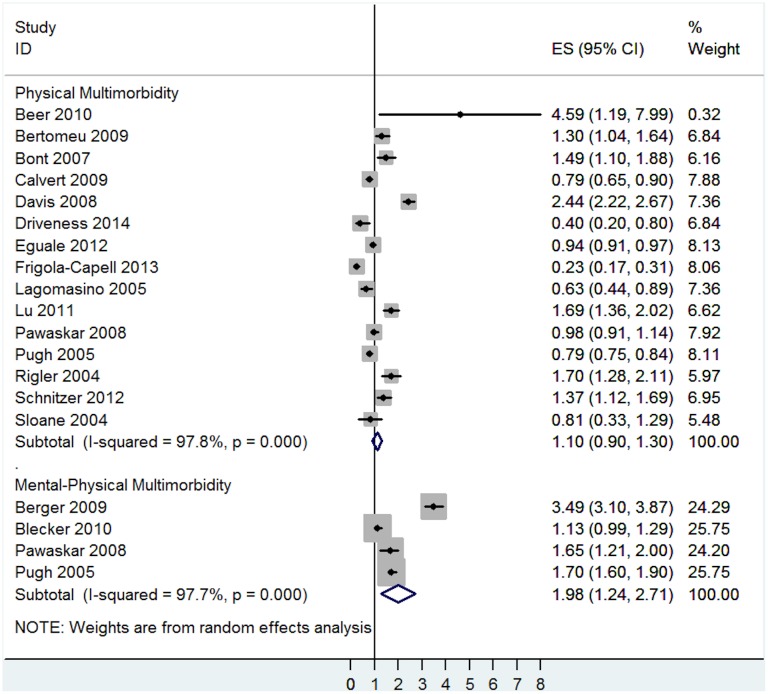
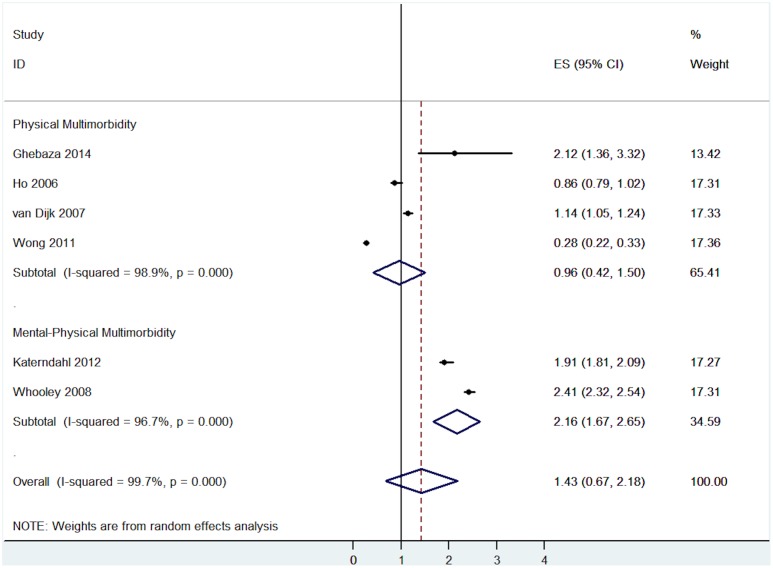
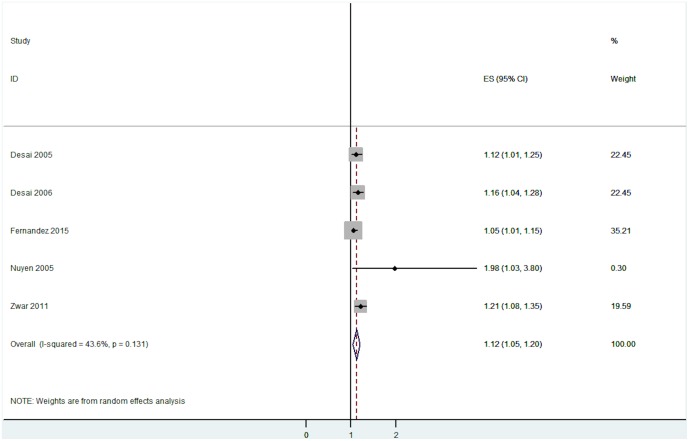
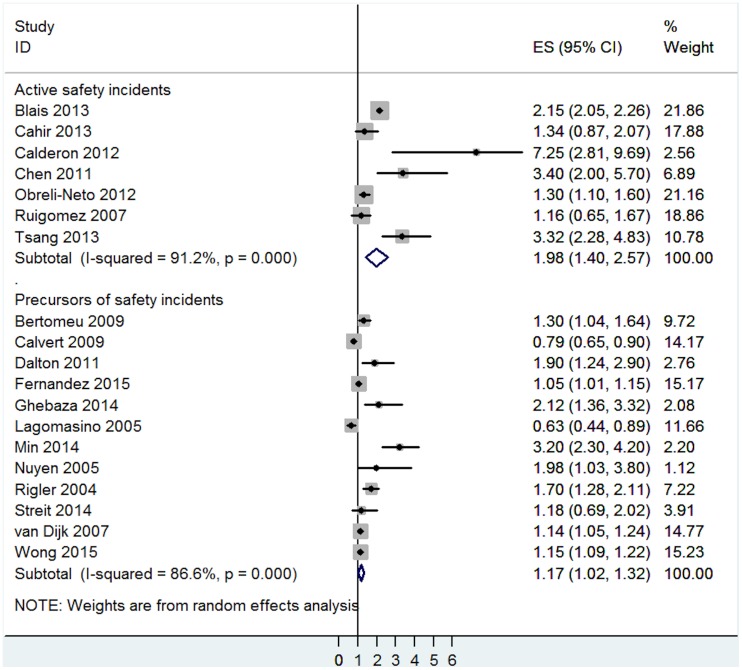
Results: Eighty six relevant comparisons from 75 studies were included in the analysis. Meta-analysis demonstrated that physical-mental multimorbidity was associated with an increased risk for 'active patient safety incidents' (OR = 2.39, 95% CI = 1.40 to 3.38) and 'precursors of safety incidents' (OR = 1.69, 95% CI = 1.36 to 2.03). Physical multimorbidity was associated with an increased risk for active safety incidents (OR = 1.63, 95% CI = 1.45 to 1.80) but was not associated with precursors of safety incidents (OR = 1.02, 95% CI = 0.90 to 1.13). Statistical heterogeneity was high and the methodological quality of the studies was generally low.
Conclusions: The association between multimorbidity and patient safety is complex, and varies by type of multimorbidity and type of safety incident. Our analyses suggest that multimorbidity involving mental health may be a key driver of safety incidents, which has important implication for the design and targeting of interventions to improve safety. High quality studies examining the mechanisms of patient safety incidents in patients with multimorbidity are needed, with the goal of promoting effective service delivery and ameliorating threats to safety in this group of patients.
Conflict of interest statement
Figures
References
-
- Department of Health: Our health, our care, our say: a new direction for community services. London: 2006.
-
- Vincent C. Patient Safety. Edinburgh: Churchill Livingstone; 2005.
-
- Klemp K. Report on a taxonomy for errors in primary care. Wolfgang Goethe University: 2009.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
