

Improving Assessment of Lipoprotein Profile in Type 1 Diabetes by 1H NMR Spectroscopy
- PMID: 26317989
- PMCID: PMC4552656
- DOI: 10.1371/journal.pone.0136348
Improving Assessment of Lipoprotein Profile in Type 1 Diabetes by 1H NMR Spectroscopy
Abstract
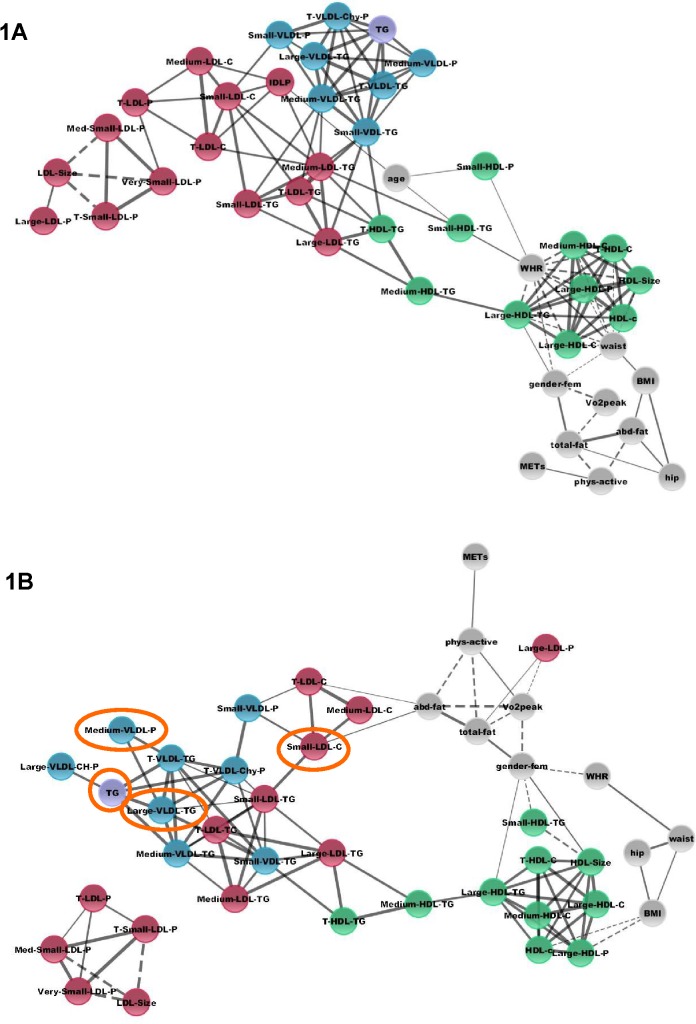
Patients with type 1 diabetes (T1D) present increased risk of cardiovascular disease (CVD). The aim of this study is to improve the assessment of lipoprotein profile in patients with T1D by using a robust developed method 1H nuclear magnetic resonance spectroscopy (1H NMR), for further correlation with clinical factors associated to CVD. Thirty patients with T1D and 30 non-diabetes control (CT) subjects, matched for gender, age, body composition (DXA, BMI, waist/hip ratio), regular physical activity levels and cardiorespiratory capacity (VO2peak), were analyzed. Dietary records and routine lipids were assessed. Serum lipoprotein particle subfractions, particle sizes, and cholesterol and triglycerides subfractions were analyzed by 1H NMR. It was evidenced that subjects with T1D presented lower concentrations of small LDL cholesterol, medium VLDL particles, large VLDL triglycerides, and total triglycerides as compared to CT subjects. Women with T1D presented a positive association with HDL size (p<0.005; R = 0.601) and large HDL triglycerides (p<0.005; R = 0.534) and negative (p<0.005; R = -0.586) to small HDL triglycerides. Body fat composition represented an important factor independently of normal BMI, with large LDL particles presenting a positive correlation to total body fat (p<0.005; R = 0.505), and total LDL cholesterol and small LDL cholesterol a positive correlation (p<0.005; R = 0.502 and R = 0.552, respectively) to abdominal fat in T1D subjects; meanwhile, in CT subjects, body fat composition was mainly associated to HDL subclasses. VO2peak was negatively associated (p<0.005; R = -0.520) to large LDL-particles only in the group of patients with T1D. In conclusion, patients with T1D with adequate glycemic control and BMI and without chronic complications presented a more favourable lipoprotein profile as compared to control counterparts. In addition, slight alterations in BMI and/or body fat composition showed to be relevant to provoking alterations in lipoproteins profiles. Finally, body fat composition appears to be a determinant for cardioprotector lipoprotein profile.
Conflict of interest statement
Figures
References
-
- American Hearth Association. Third report of the National Education Program (NCEP) Expert Panel on Detection, Evaluation, and Treatment of High Bloos Cholesterol in Adults (Adult Treatment Panell III) Final Report. Circulation. 2002;106:3143–3421. - PubMed
-
- Laing SP, Swerdlow AJ, Slater SD, Burden AC, Morris A, Waugh NR et al. Mortality from heart disease in a cohort of 23,000 patients with insulin-treated diabetes. Diabetologia. 2003;46:760–5. - PubMed
-
- Soedamah-Muthu SS, Fuller JH, Mulnier HE, Raleigh VS, Lawrenson RA, Colhoun HM. All-cause mortality rates in patients with type 1 diabetes mellitus compared with a non-diabetic population from the UK general practice research database, 1992–1999. Diabetologia. 2006;49:660–6. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
