

Non-invasive measurements of pulse pressure variation and stroke volume variation in anesthetized patients using the Nexfin blood pressure monitor
- PMID: 26318314
- PMCID: PMC5023739
- DOI: 10.1007/s10877-015-9759-7
Non-invasive measurements of pulse pressure variation and stroke volume variation in anesthetized patients using the Nexfin blood pressure monitor
Abstract
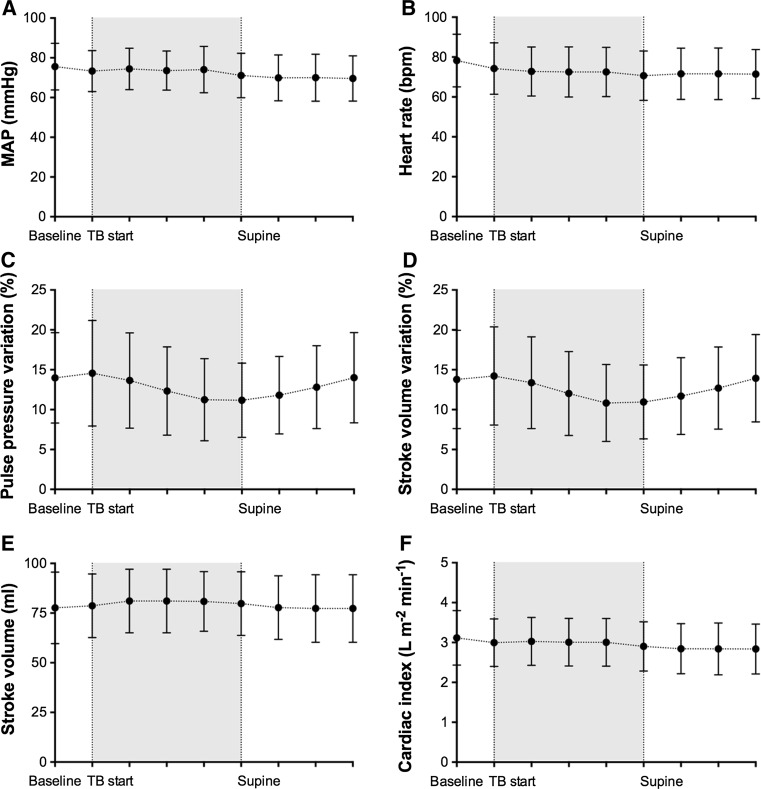
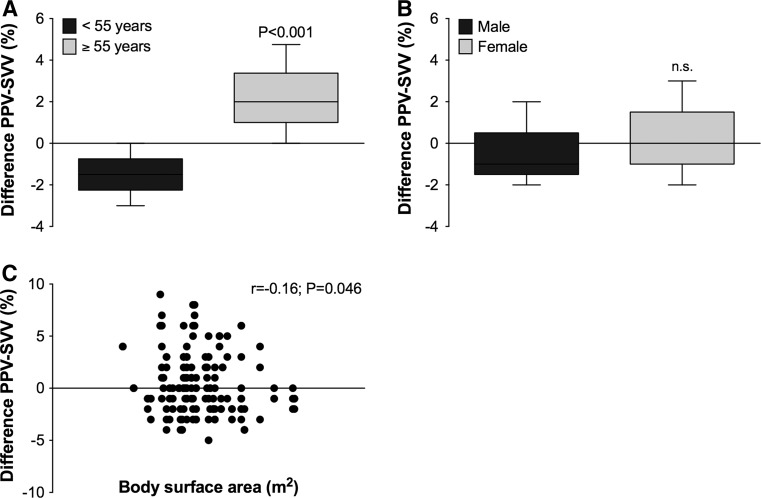
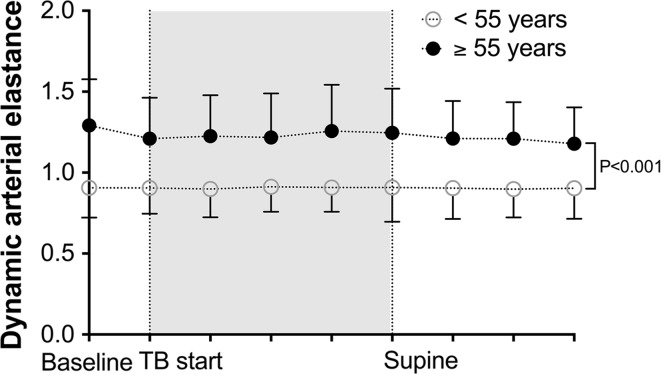
Nexfin beat-to-beat arterial blood pressure monitoring enables continuous assessment of hemodynamic indices like cardiac index (CI), pulse pressure variation (PPV) and stroke volume variation (SVV) in the perioperative setting. In this study we investigated whether Nexfin adequately reflects alterations in these hemodynamic parameters during a provoked fluid shift in anesthetized and mechanically ventilated patients. The study included 54 patients undergoing non-thoracic surgery with positive pressure mechanical ventilation. The provoked fluid shift comprised 15° Trendelenburg positioning, and fluid responsiveness was defined as a concomitant increase in stroke volume (SV) >10 %. Nexfin blood pressure measurements were performed during supine steady state, Trendelenburg and supine repositioning. Hemodynamic parameters included arterial blood pressure (MAP), CI, PPV and SVV. Trendelenburg positioning did not affect MAP or CI, but induced a decrease in PPV and SVV by 3.3 ± 2.8 and 3.4 ± 2.7 %, respectively. PPV and SVV returned back to baseline values after repositioning of the patient to baseline. Bland-Altman analysis of SVV and PPV showed a bias of -0.3 ± 3.0 % with limits of agreement ranging from -5.6 to 6.2 %. The SVV was more superior in predicting fluid responsiveness (AUC 0.728) than the PVV (AUC 0.636), respectively. The median bias between PPV and SVV was different for patients younger [-1.5 % (-3 to 0)] or older [+2 % (0-4.75)] than 55 years (P < 0.001), while there were no gender differences in the bias between PPV and SVV. The Nexfin monitor adequately reflects alterations in PPV and SVV during a provoked fluid shift, but the level of agreement between PPV and SVV was low. The SVV tended to be superior over PPV or Eadyn in predicting fluid responsiveness in our population.
Keywords: Anesthesia; Blood pressure; Cardiac output; Fluid challenge; Hemodynamic; Non-invasive monitoring.
Conflict of interest statement
The authors declare that they have no conflict of interest. Ethical approval All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Figures

References
-
- Cecconi M, Monti G, Hamilton MA, et al. Efficacy of functional hemodynamic parameters in predicting fluid responsiveness with pulse power analysis in surgical patients. Minerva Anestesiol. 2012;78:527–533. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
