

Cardiovascular magnetic resonance predictors of clinical outcome in patients with suspected acute myocarditis
- PMID: 26318624
- PMCID: PMC4553007
- DOI: 10.1186/s12968-015-0185-2
Cardiovascular magnetic resonance predictors of clinical outcome in patients with suspected acute myocarditis
Abstract
Background: The natural history of acute myocarditis (AM) remains highly variable and predictors of outcome are largely unknown. The objectives were to determine the potential value of various cardiovascular magnetic resonance (CMR) parameters for the prediction of adverse long-term outcome in patients presenting with suspected AM.
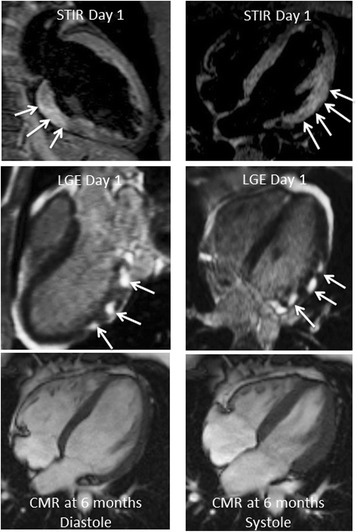
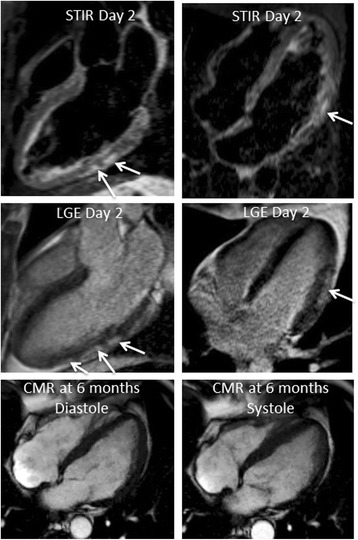
Methods: In a single-centre longitudinal prospective study, 203 routine consecutive patients with an initial CMR-based diagnosis of AM (typical Late Gadolinium Enhancement, LGE) were followed over a mean period of 18.9 ± 8.2 months. Various CMR parameters were evaluated as potential predictors of outcome. The primary endpoint was defined as the occurrence of at least one of the combined Major Adverse Clinical Events (MACE) (cardiac death or aborted sudden cardiac death, cardiac transplantation, sustained documented ventricular tachycardia, heart failure, recurrence of acute myocarditis, and the need for hospitalization for cardiac causes).
Results: The vast majority of patients (N = 143,70 %) presented with chest pain, mild to moderate troponin elevation and ST-segment or T wave abnormalities. Various CMR parameters were evaluated on initial CMR performed 3 ± 2 days after acute clinical presentation (LV functional parameters, presence/extent of edema on T2 CMR, and extent of late gadolinium enhancement lesions). Out of the 203 patients, 22 experienced at least one major cardiovascular event (10.8 %) during follow-up for a total of 31 major cardiovascular events. Among all CMR parameters, the only independent CMR predictor of adverse clinical outcome by multivariate analysis was an initial alteration of LVEF (p = 0.04).
Conclusions: In routine consecutive patients without severe hemodynamic compromise and a CMR-based diagnosis of AM, various CMR parameters such as the presence and extent of myocardial edema and the extent of late gadolinium-enhanced LV myocardial lesions were not predictive of outcome. The only independent CMR predictor of adverse clinical outcome was an initial alteration of LVEF.
Figures
References
-
- Liu P, Kenneth L, Baughman KL. Myocarditis. Braunwald’s Heart Disease. A Textbook of Cardiovascular Medicine. 9th edition. Cambridge, MA: Saunders Elsevier; 2011:1595-1609.
-
- Doolan A, Langlois N, Semsarian C. Causes of sudden cardiac death in young Australians. Med J Aust. 2004;180:110–2. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
