

An illustrative overview of semi-quantitative MRI scoring of knee osteoarthritis: lessons learned from longitudinal observational studies
- PMID: 26318656
- PMCID: PMC4724524
- DOI: 10.1016/j.joca.2015.08.011
An illustrative overview of semi-quantitative MRI scoring of knee osteoarthritis: lessons learned from longitudinal observational studies
Abstract
Objective: To introduce the most popular magnetic resonance imaging (MRI) osteoarthritis (OA) semi-quantitative (SQ) scoring systems to a broader audience with a focus on the most commonly applied scores, i.e., the MOAKS and WORMS system and illustrate similarities and differences.
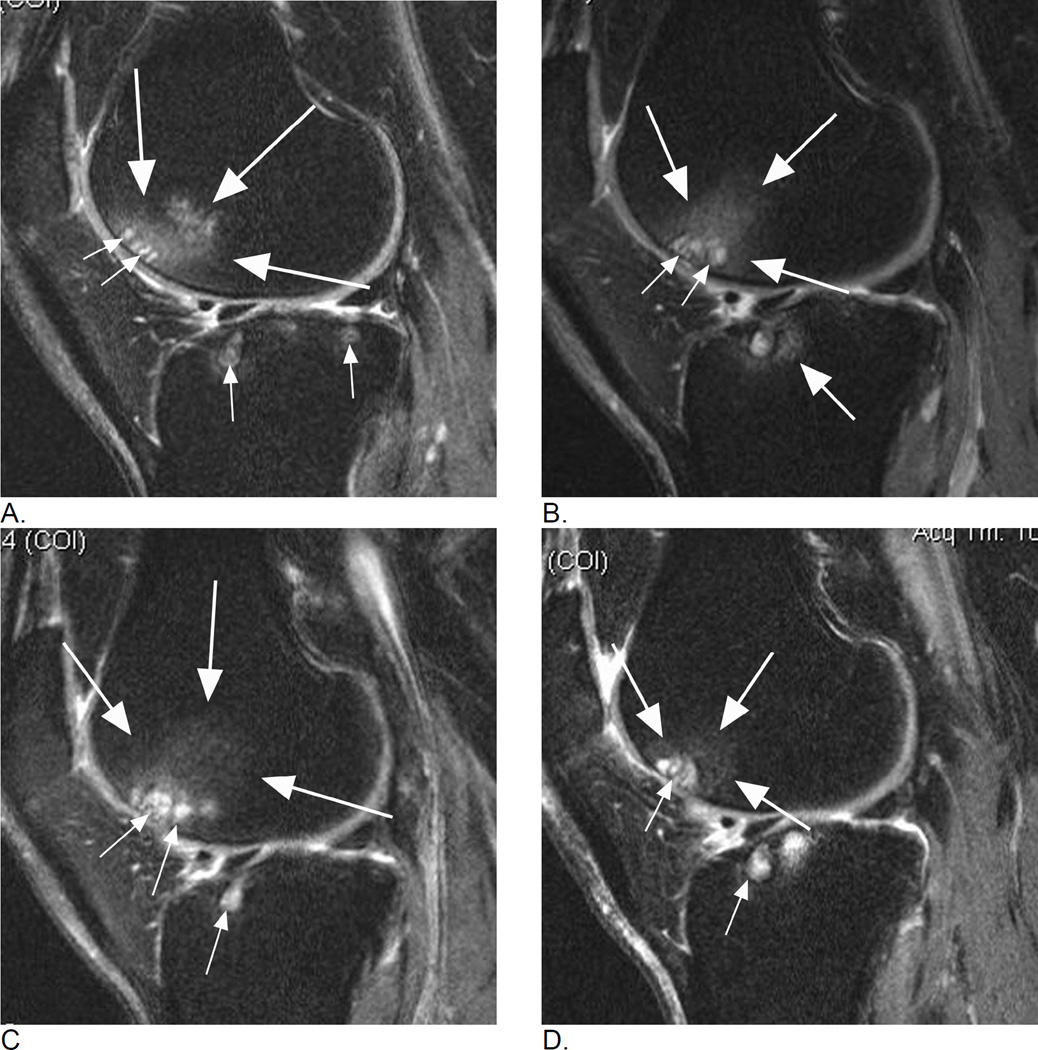
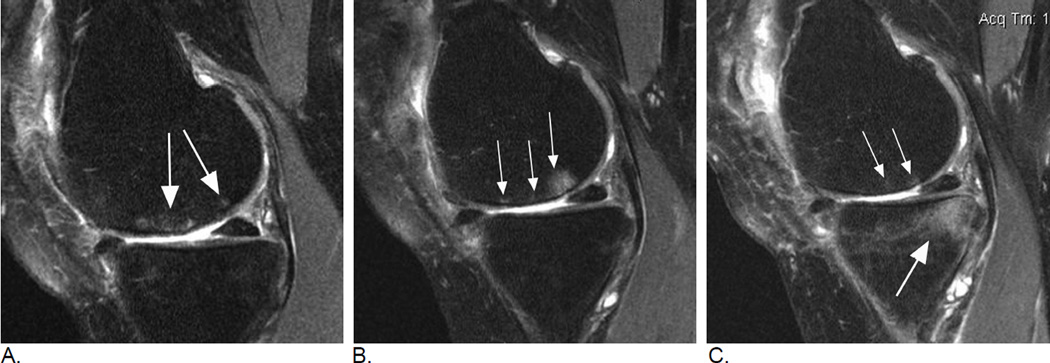
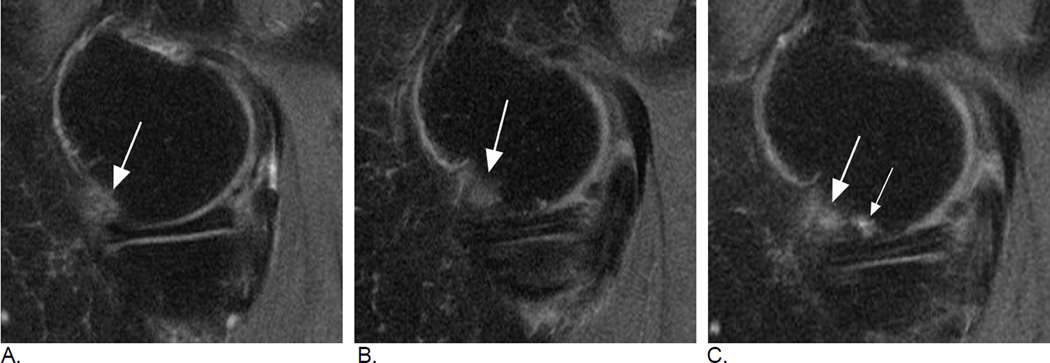
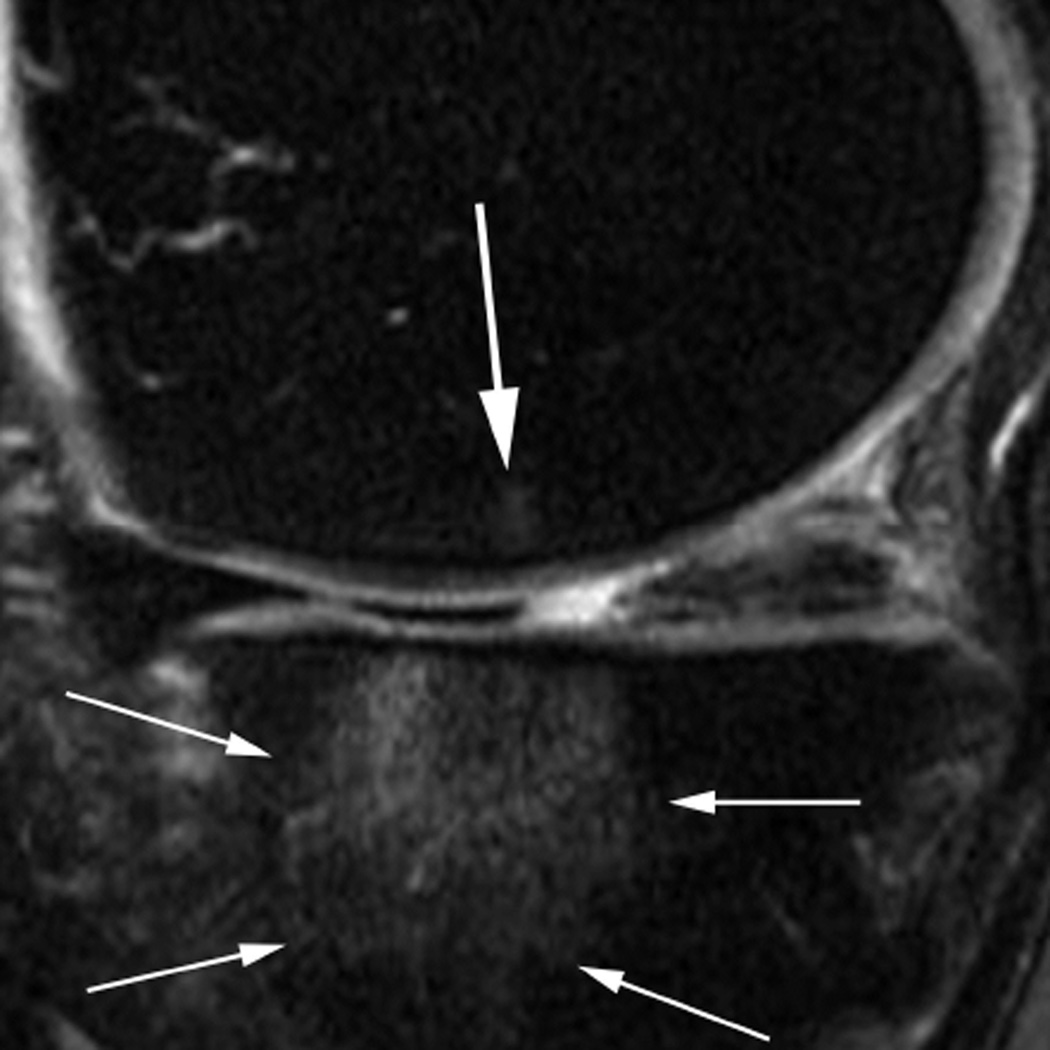
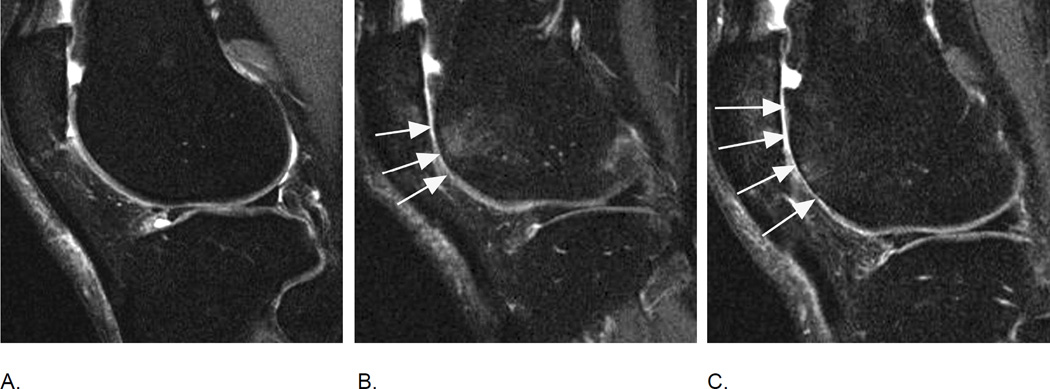
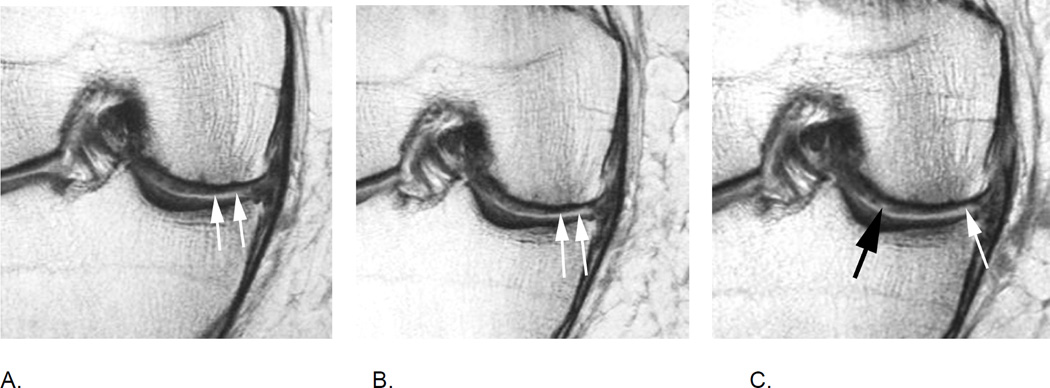
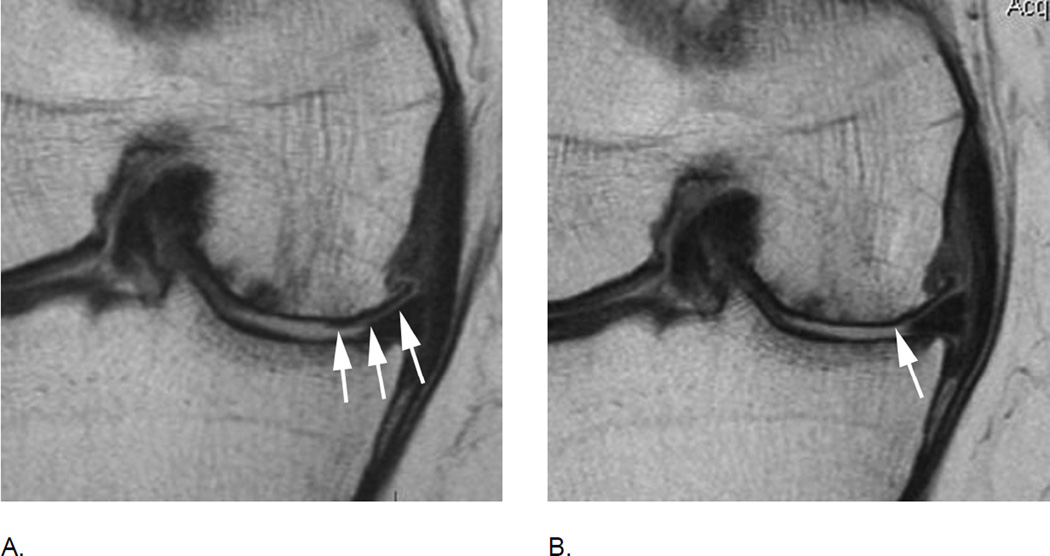
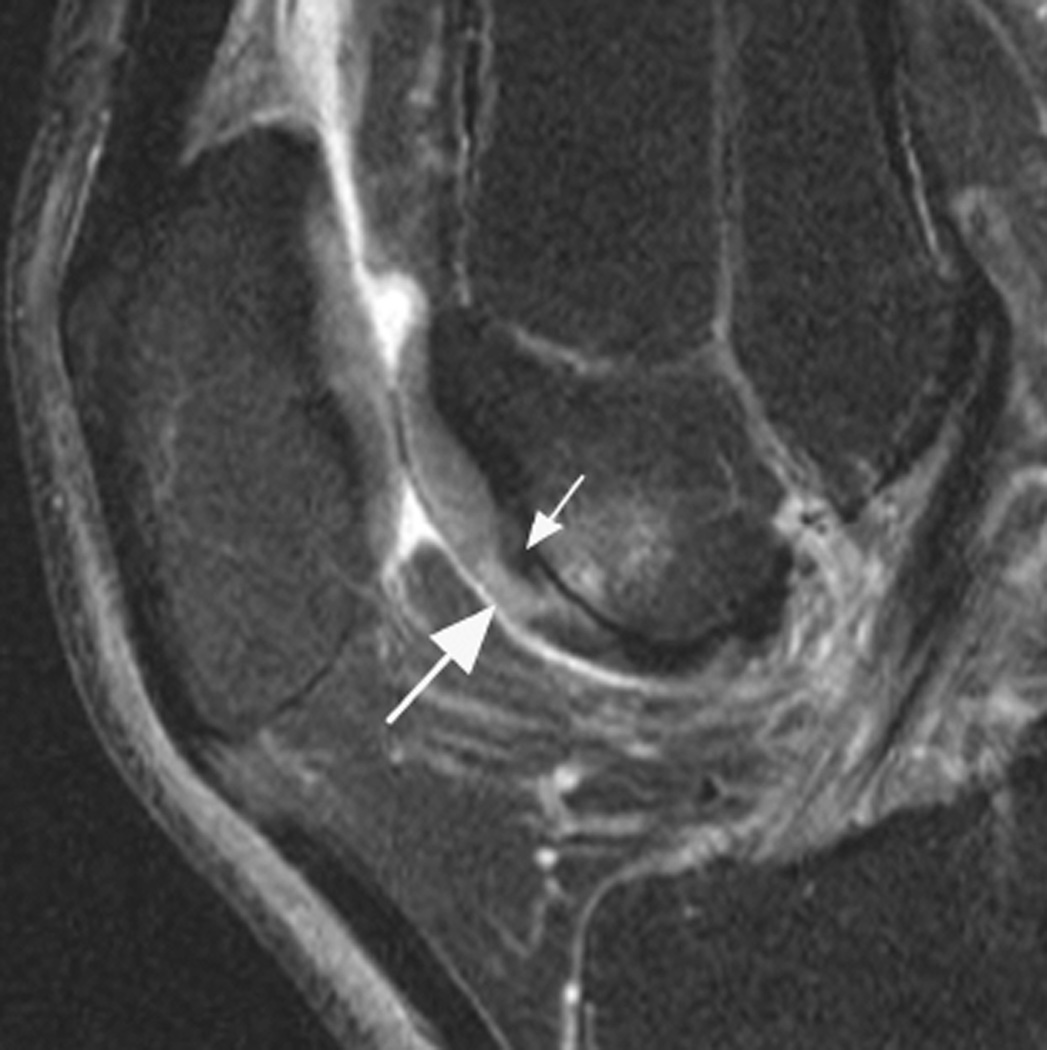
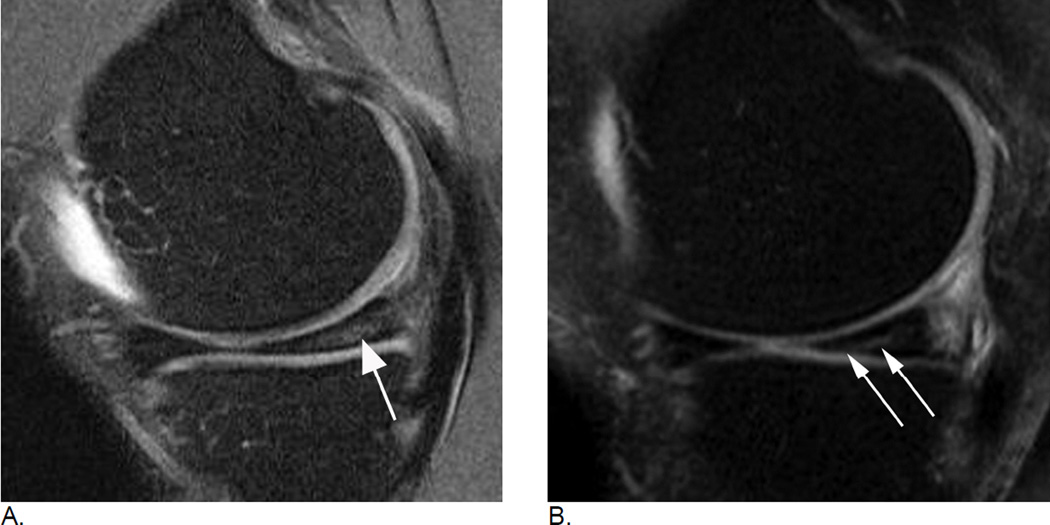
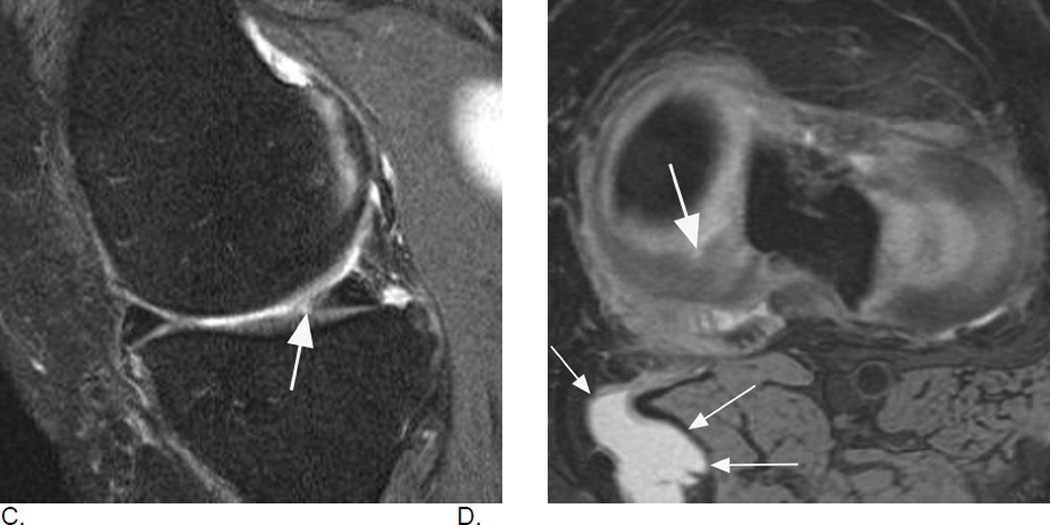
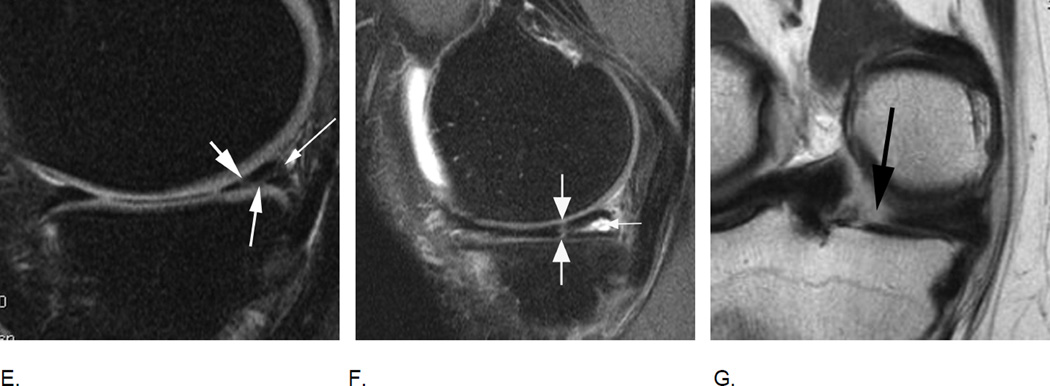
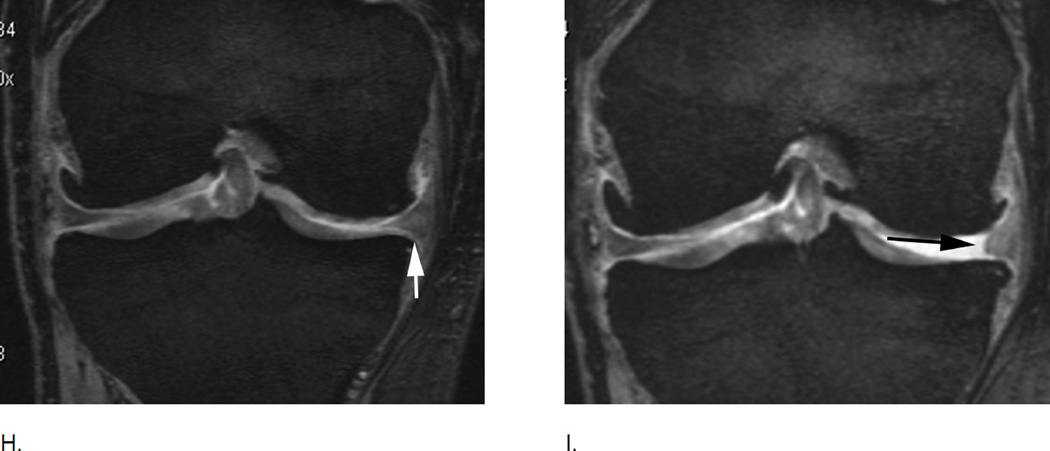
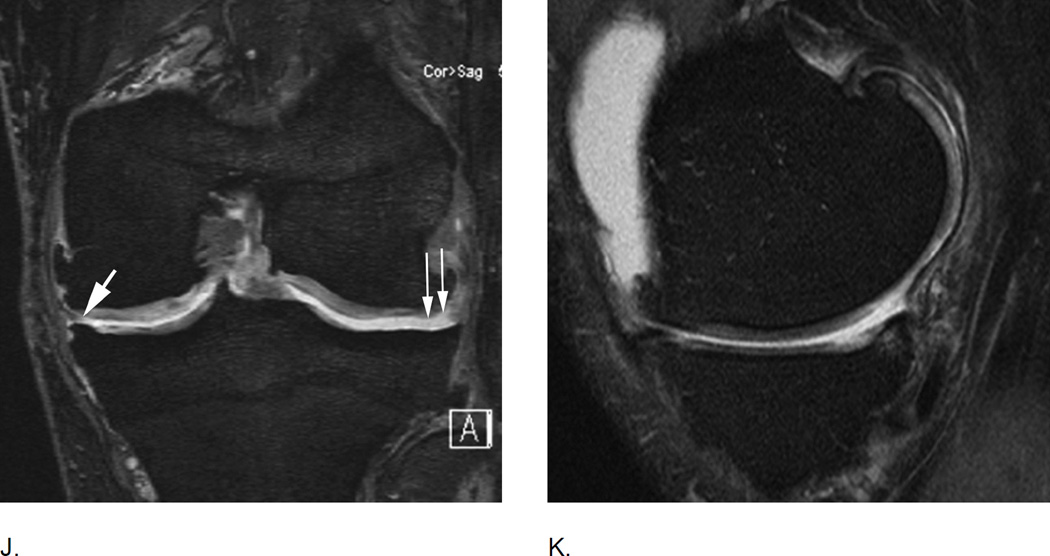
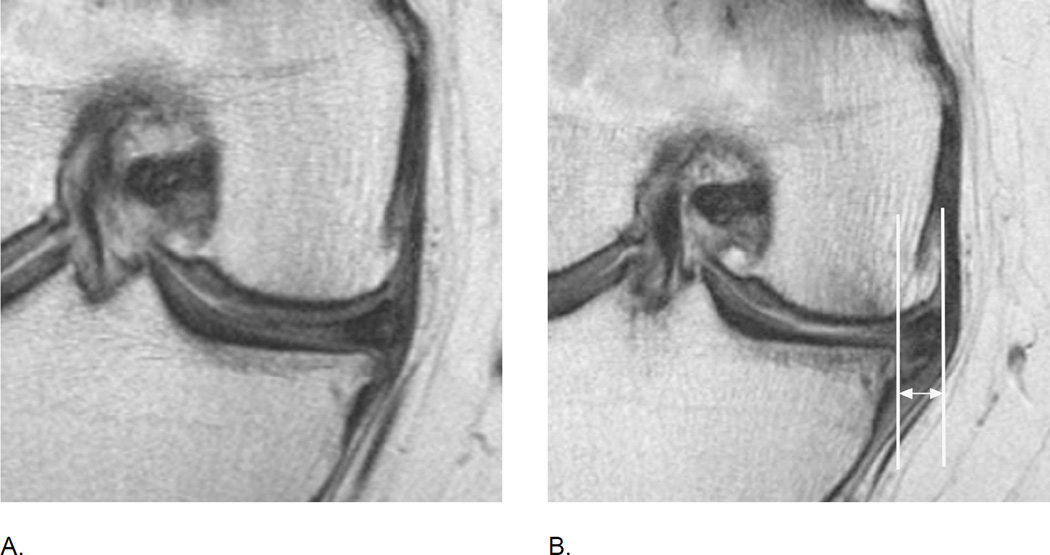
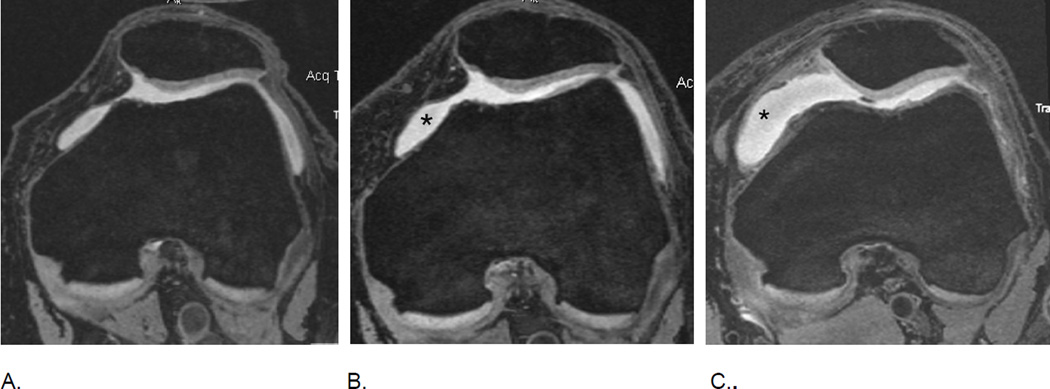
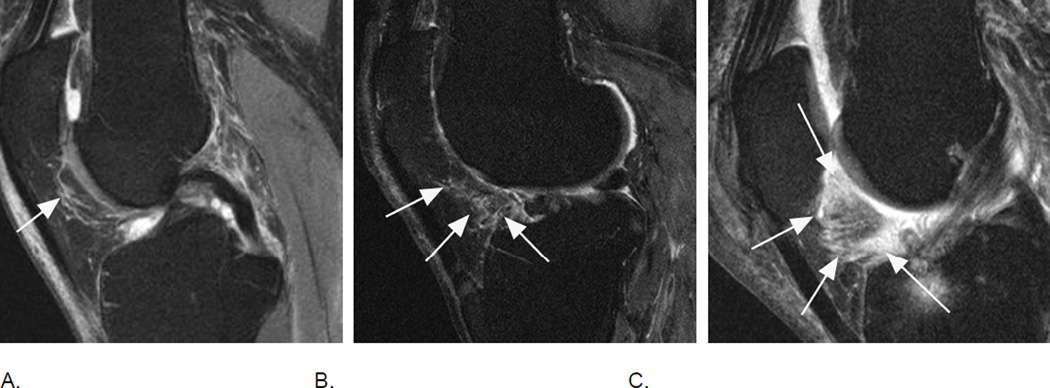
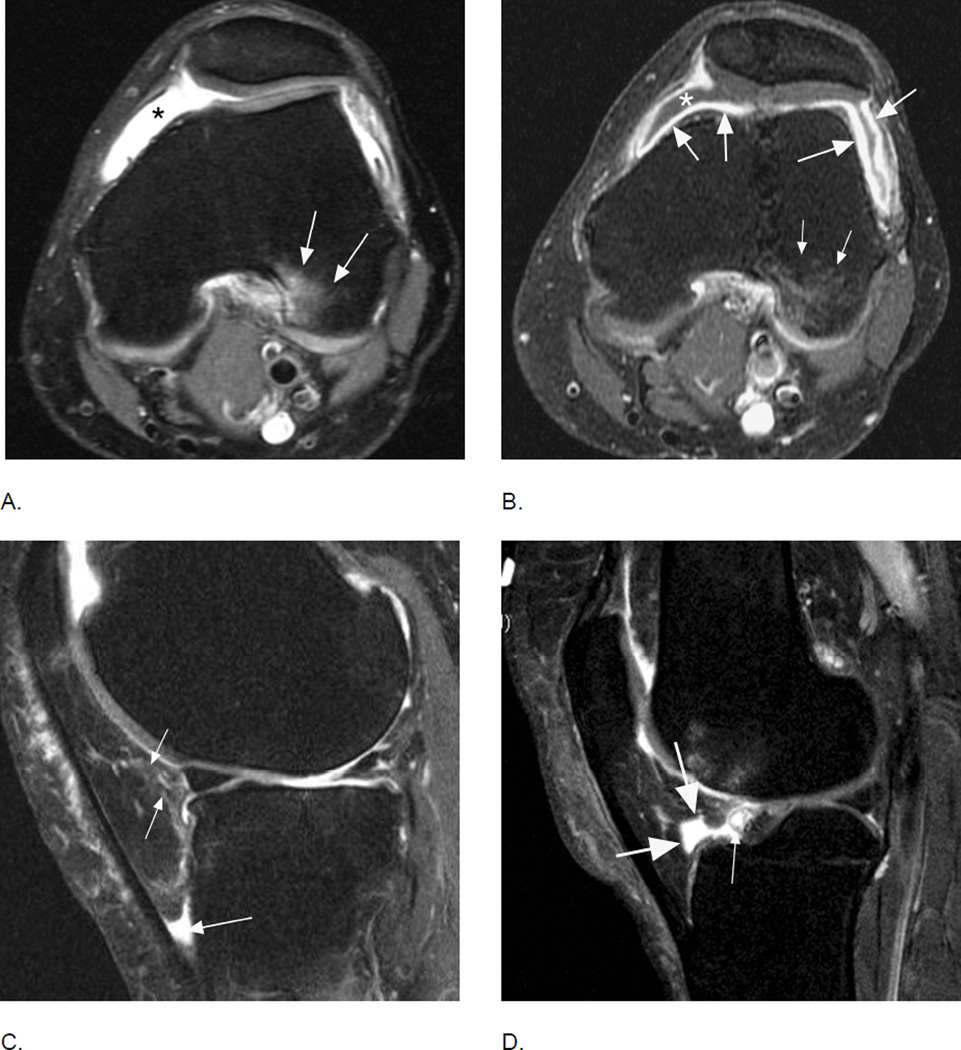
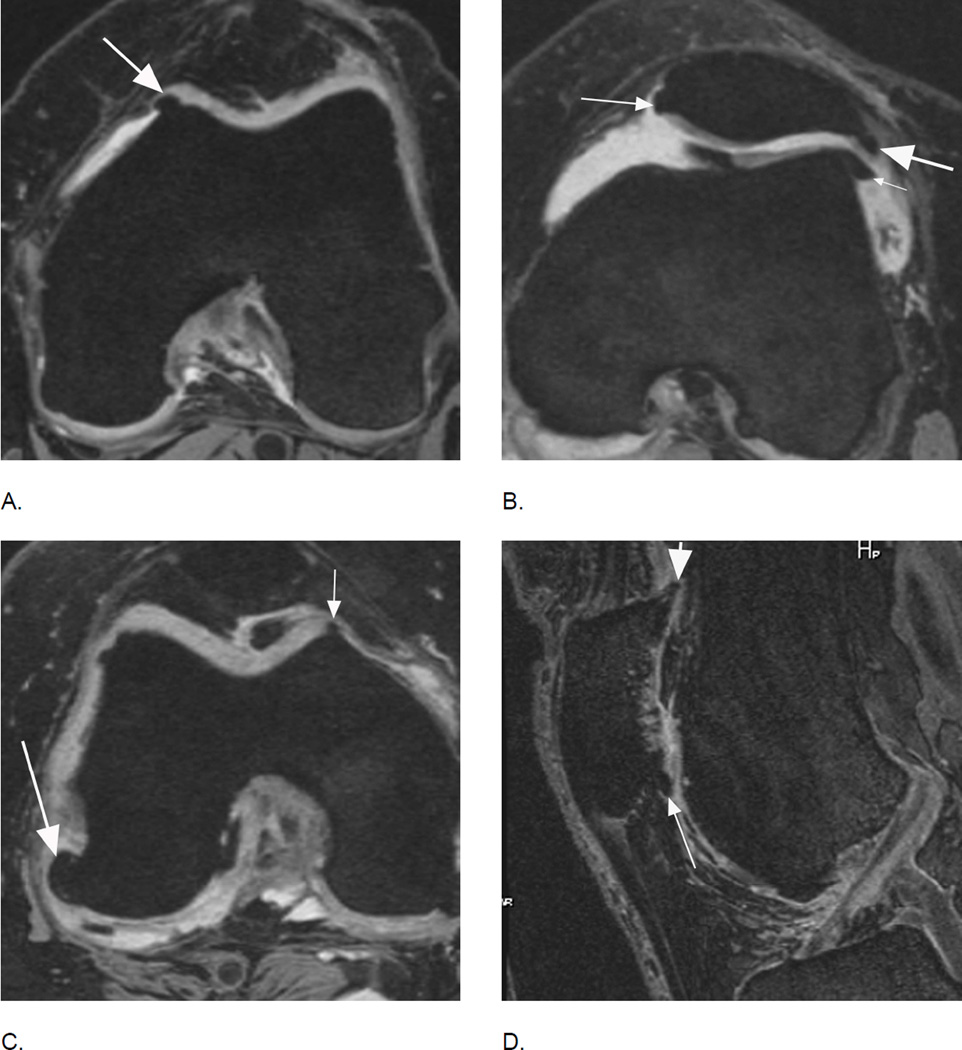
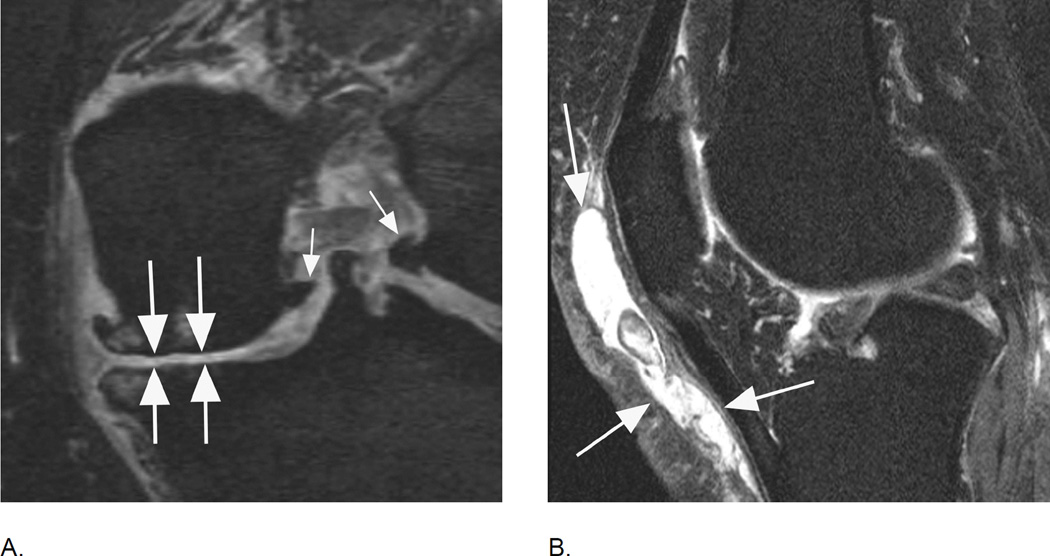
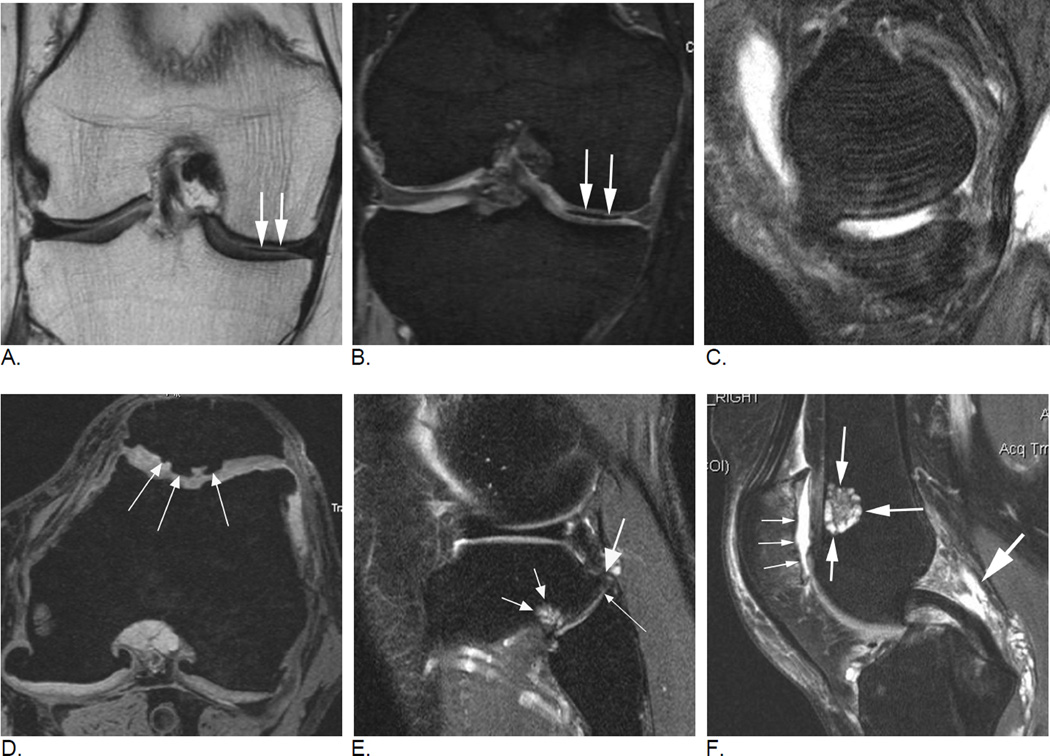
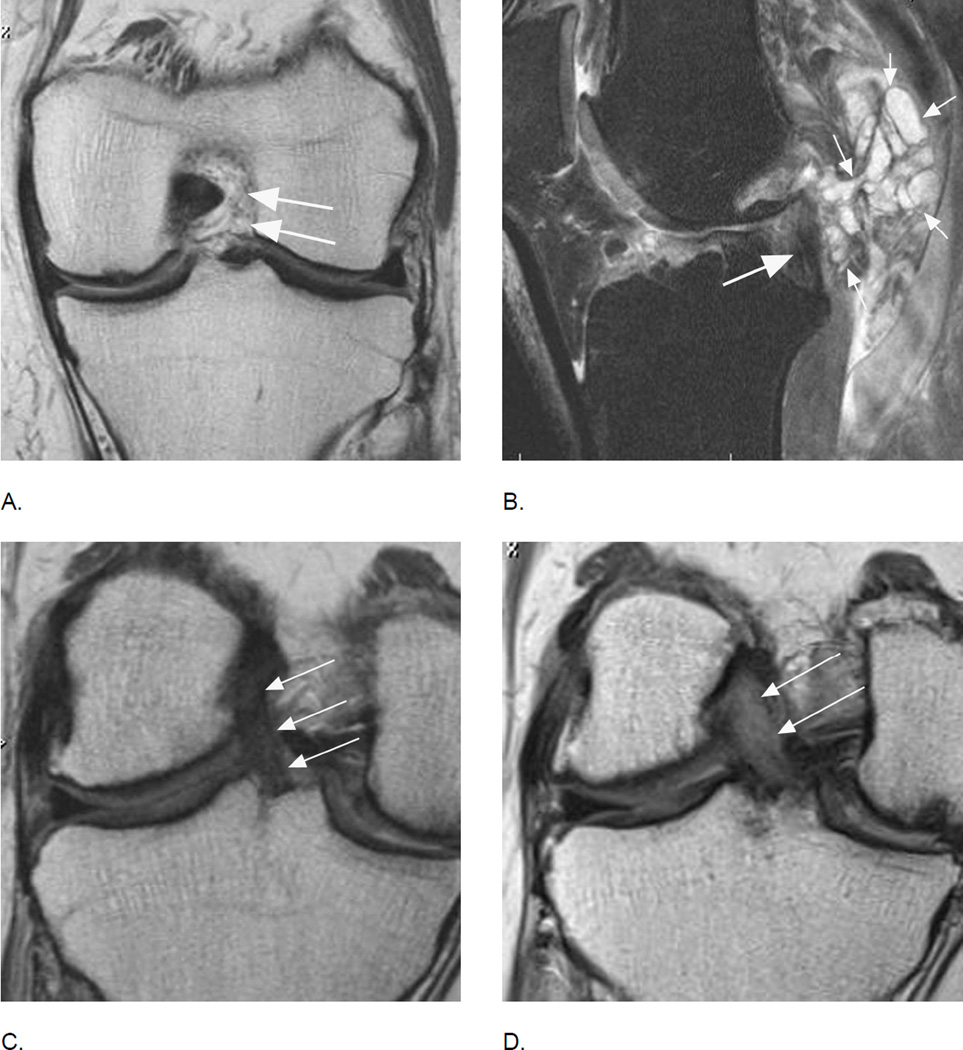
Design: While the main structure and methodology of each scoring system are publicly available, the core of this overview will be an illustrative imaging atlas section including image examples from multiple OA studies applying MRI in regard to different features assessed, show specific examples of different grades and point out pitfalls and specifics of SQ assessment including artifacts, blinding to time point of acquisition and within-grade evaluation.
Results: Similarities and differences between different scoring systems are presented. Technical considerations are followed by a brief description of the most commonly utilized SQ scoring systems including their responsiveness and reliability. The second part is comprised of the atlas section presenting illustrative image examples.
Conclusions: Evidence suggests that SQ assessment of OA by expert MRI readers is valid, reliable and responsive, which helps investigators to understand the natural history of this complex disease and to evaluate potential new drugs in OA clinical trials. Researchers have to be aware of the differences and specifics of the different systems to be able to engage in imaging assessment and interpretation of imaging-based data. SQ scoring has enabled us to explain associations of structural tissue damage with clinical manifestations of the disease and with morphological alterations thought to represent disease progression.
Keywords: Imaging; MOAKS; MRI; Osteoarthritis; Semi-quantitative scoring; WORMS.
Copyright © 2015 Osteoarthritis Research Society International. Published by Elsevier Ltd. All rights reserved.
Figures




References
-
- Peterfy CG, Guermazi A, Zaim S, Tirman PF, Miaux Y, White D, et al. Whole-Organ Magnetic Resonance Imaging Score (WORMS) of the knee in osteoarthritis. Osteoarthritis Cartilage. 2004;12:177–190. - PubMed
-
- Guermazi A, Roemer FW, Haugen IK, Crema MD, Hayashi D. MRI-based semiquantitative scoring of joint pathology in osteoarthritis. Nat Rev Rheumatol. 2013;9:236–251. - PubMed
-
- Kornaat PR, Ceulemans RY, Kroon HM, Riyazi N, Kloppenburg M, Carter WO, et al. MRI assessment of knee osteoarthritis: Knee Osteoarthritis Scoring System (KOSS)--inter-observer and intra-observer reproducibility of a compartment-based scoring system. Skeletal Radiol. 2005;34:95–102. - PubMed
-
- Hunter DJ, Lo GH, Gale D, Grainger AJ, Guermazi A, Conaghan PG. The reliability of a new scoring system for knee osteoarthritis MRI and the validity of bone marrow lesion assessment: BLOKS (Boston Leeds Osteoarthritis Knee Score) Ann Rheum Dis. 2008;67:206–211. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
