

The Role of Surgical Resection in Stage IIIA Non-Small Cell Lung Cancer: A Decision and Cost-Effectiveness Analysis
- PMID: 26319488
- PMCID: PMC4847712
- DOI: 10.1016/j.athoracsur.2015.05.091
The Role of Surgical Resection in Stage IIIA Non-Small Cell Lung Cancer: A Decision and Cost-Effectiveness Analysis
Abstract
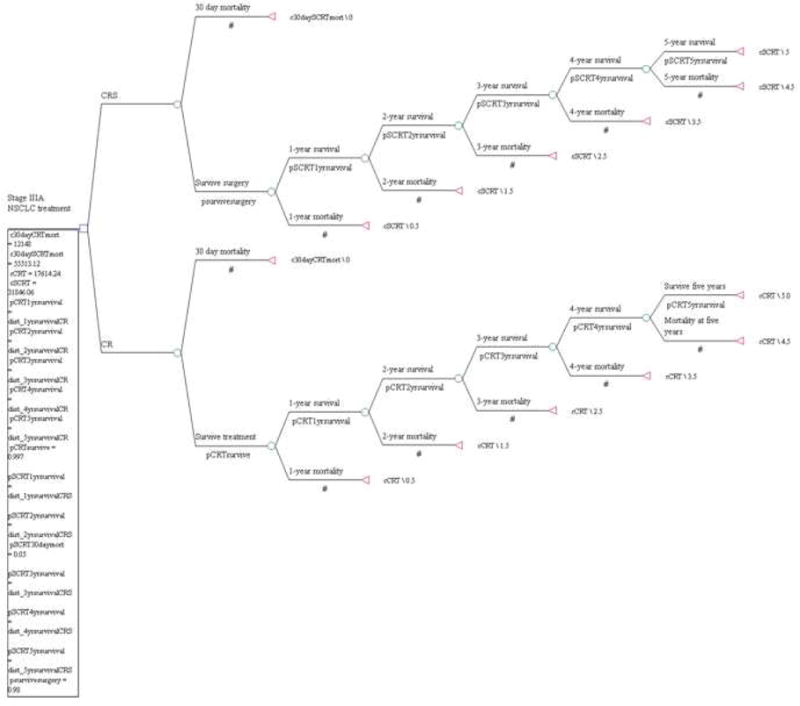
Background: This study evaluated the cost-effectiveness of combination chemotherapy, radiotherapy, and surgical intervention (CRS) vs definitive chemotherapy and radiotherapy (CR) in clinical stage IIIA non-small cell lung cancer (NSCLC) patients at academic and nonacademic centers.
Methods: Patients with clinical stage IIIA NSCLC receiving CR or CRS from 1998 to 2010 were identified in the National Cancer Data Base. Propensity score matching on patient, tumor, and treatment characteristics was performed. Medicare allowable charges were used for treatment costs. The incremental cost-effectiveness ratio (ICER) was based on probabilistic 5-year survival and calculated as cost per life-year gained.
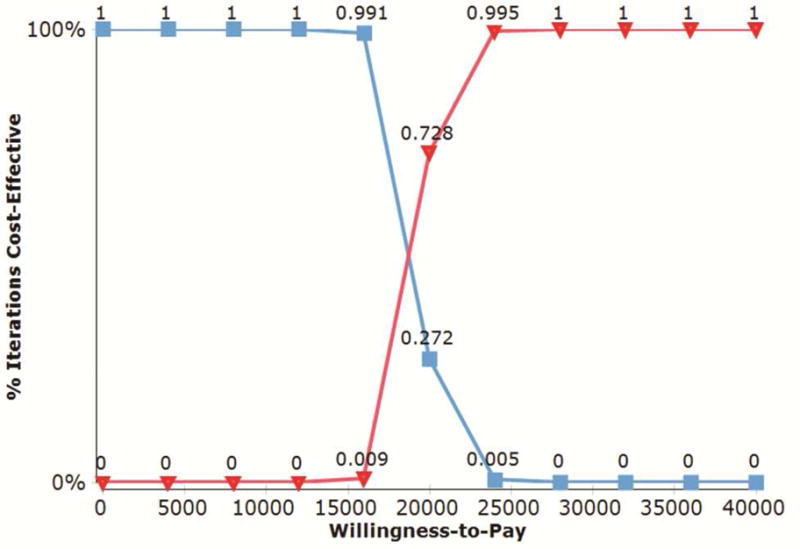
Results: We identified 5,265 CR and CRS matched patient pairs. Surgical resection imparted an increased effectiveness of 0.83 life-years, with an ICER of $17,618. Among nonacademic centers, 1,634 matched CR and CRS patients demonstrated a benefit with surgical resection of 0.86 life-years gained, for an ICER of $17,124. At academic centers, 3,201 matched CR and CRS patients had increased survival of 0.81 life-years with surgical resection, for an ICER of $18,144. Finally, 3,713 CRS patients were matched between academic and nonacademic centers. Academic center surgical patients had an increased effectiveness of 1.5 months gained and dominated the model with lower surgical cost estimates associated with lower 30-day mortality rates.
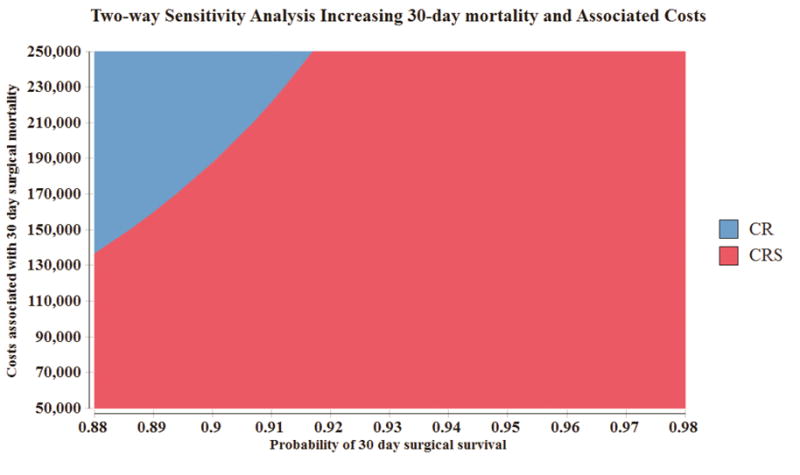
Conclusions: In stage IIIA NSCLC, the selective addition of surgical resection to CR is cost-effective compared with definitive chemoradiation therapy at nonacademic and academic centers. These conclusions are valid over a range of clinically meaningful variations in cost and treatment outcomes.
Copyright © 2015 The Society of Thoracic Surgeons. Published by Elsevier Inc. All rights reserved.
Figures
References
-
- Yabroff KR, Lamont EB, Mariotto A, et al. Cost of care for elderly cancer patients in the United States. J Natl Cancer Inst. 2008;100:630–641. - PubMed
-
- Keehan S, Sisko A, Truffer C, et al. Health spending projections through 2017: the baby-boom generation is coming to Medicare. Health Aff (Millwood) 2008;27:w145–155. - PubMed
-
- Morgensztern D, Waqar S, Subramanian J, et al. Prognostic significance of tumor size in patients with stage III non-small-cell lung cancer: a surveillance, epidemiology, and end results (SEER) survey from 1998 to 2003. J Thorac Oncol. 2012;7:1479–1484. - PubMed
-
- Groome PA, Bolejack V, Crowley JJ, et al. The IASLC Lung Cancer Staging Project: validation of the proposals for revision of the T, N, and M descriptors and consequent stage groupings in the forthcoming (seventh) edition of the TNM classification of malignant tumours. J Thorac Oncol. 2007;2:694–705. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
