

LV Mass as a Predictor of CVD Events in Older Adults With and Without Metabolic Syndrome and Diabetes
- PMID: 26319502
- PMCID: PMC5845438
- DOI: 10.1016/j.jcmg.2015.04.019
LV Mass as a Predictor of CVD Events in Older Adults With and Without Metabolic Syndrome and Diabetes
Abstract
Objectives: The purpose of this study was to examine the prognostic significance of left ventricular (LV) mass for cardiovascular disease (CVD) events in older adults with and without metabolic syndrome (MetS) and diabetes mellitus (DM).
Background: MetS and DM are associated with increased CVD risk, but it is unclear in these groups whether subclinical CVD as shown by increased LV mass improves risk prediction compared to standard risk factors in older individuals.
Methods: We studied 3,724 adults (mean 72.4 ± 5.4 years of age, 61.0% female, 4.4% African-American) from the Cardiovascular Health Study who had MetS but not DM or had DM alone or had neither condition. Cox regression was used to examine the association of LV mass, (alone and indexed by height and body surface area [BSA]) as determined by echocardiography, with CVD events, including coronary heart disease (CHD), stroke, heart failure (HF), and CVD death, as well as total mortality. We also assessed the added prediction, discriminative value, and net reclassification improvement (NRI) for clinical utility of LV mass compared to standard risk factors.
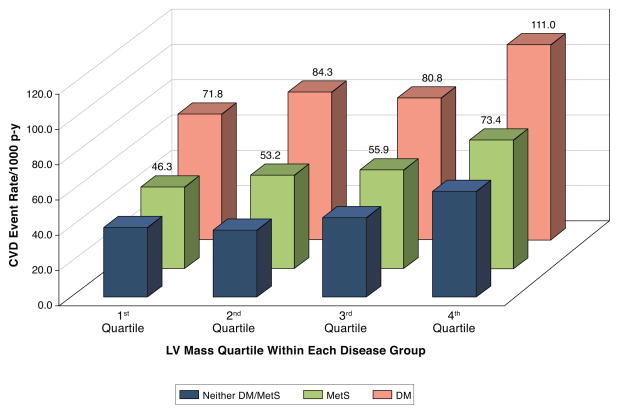
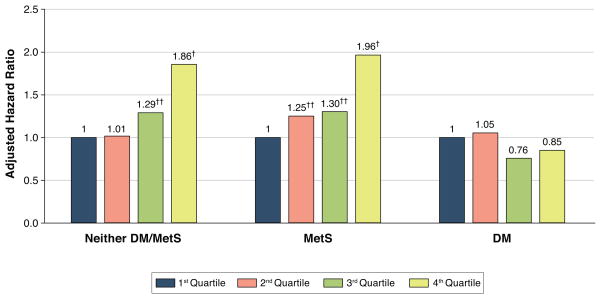
Results: Over a mean follow-up of 14.2 ± 6.3 years, 2,180 subjects experienced CVD events, including 986 CVD deaths. After adjustment for age, sex and standard risk factors, LV mass was positively associated with CVD events in those with MetS (hazard ratio [HR]: 1.4, p < 0.001) and without MetS (HR: 1.4, p < 0.001), but not DM (HR: 1.0, p = 0.62), with similar findings for LV mass indexed for height or BSA. Adding LV mass to standard risk factors moderately improved the prediction accuracy in the overall sample and MetS group from changes in C-statistics (p < 0.05). Categorical-free net reclassification improvement increased significantly by 17% to 19% in those with MetS. Findings were comparable for CHD, CVD mortality, and total mortality.
Conclusions: LV mass is associated with increased CVD risk and provides modest added prediction and clinical utility compared to standard risk factors in older persons with and without MetS but not with DM.
Keywords: cardiovascular disease; diabetes; echocardiography; left ventricular mass; metabolic syndrome.
Copyright © 2015 American College of Cardiology Foundation. Published by Elsevier Inc. All rights reserved.
Figures
Comment in
-
Cardiac "Morphomics": Do We Need to Measure LV Mass and Geometry in Everyone?JACC Cardiovasc Imaging. 2015 Sep;8(9):1016-1018. doi: 10.1016/j.jcmg.2015.06.008. JACC Cardiovasc Imaging. 2015. PMID: 26381764 No abstract available.
References
-
- Wong ND. Metabolic syndrome: cardiovascular risk assessment and management. Am J Cardiovasc Drugs. 2007;7:259–72. - PubMed
-
- Ford ES. Risks for all-cause mortality, cardiovascular disease, and diabetes associated with the metabolic syndrome: a summary of the evidence. Diabetes Care. 2005;28:1769–1778. - PubMed
-
- Malik S, Wong ND, Franklin SS, Kamath TV, L’Italien GJ, Pio JR, Williams GR. Impact of the metabolic syndrome on mortality from coronary heart disease, cardiovascular disease, and all causes in United States adults. Circulation. 2004;110:1245–50. - PubMed
-
- Mozaffarian D, Kamineni A, Prineas RJ, Siscovick DS. Metabolic syndrome and mortality in older adults: the Cardiovascular Health Study. Arch Intern Med. 2008;168:969–78. - PubMed
-
- Gardin JM, McClelland R, Kitzman D, et al. M-mode echocardiographic predictors of six- to seven-year incidence of coronary heart disease, stroke, congestive heart failure, and mortality in an elderly cohort (The Cardiovascular Health Study) Am J Cardiol. 2001;87:1051–7. - PubMed
Publication types
MeSH terms
Grants and funding
- N01 HC085080/HL/NHLBI NIH HHS/United States
- U01 HL080295/HL/NHLBI NIH HHS/United States
- N01 HC055222/HL/NHLBI NIH HHS/United States
- N01 HC085079/HL/NHLBI NIH HHS/United States
- R01 HL080295/HL/NHLBI NIH HHS/United States
- R01 AG023629/AG/NIA NIH HHS/United States
- N01 HC085081/HL/NHLBI NIH HHS/United States
- N01 HC55222/HC/NHLBI NIH HHS/United States
- N01 HC085082/HL/NHLBI NIH HHS/United States
- HHSN268201200036C/HL/NHLBI NIH HHS/United States
- N01 HC085086/HL/NHLBI NIH HHS/United States
- N01 HC085083/HL/NHLBI NIH HHS/United States
- HL080295/HL/NHLBI NIH HHS/United States
- HHSN268200800007C/HL/NHLBI NIH HHS/United States
- AG023629/AG/NIA NIH HHS/United States
- R56 AG023629/AG/NIA NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
