

Acute Kidney Injury Incidence in Noncritically Ill Hospitalized Children, Adolescents, and Young Adults: A Retrospective Observational Study
- PMID: 26319754
- PMCID: PMC4769119
- DOI: 10.1053/j.ajkd.2015.07.019
Acute Kidney Injury Incidence in Noncritically Ill Hospitalized Children, Adolescents, and Young Adults: A Retrospective Observational Study
Abstract
Background: Acute kidney injury (AKI) has been characterized in high-risk pediatric hospital inpatients, in whom AKI is frequent and associated with increased mortality, morbidity, and length of stay. The incidence of AKI among patients not requiring intensive care is unknown.
Study design: Retrospective cohort study.
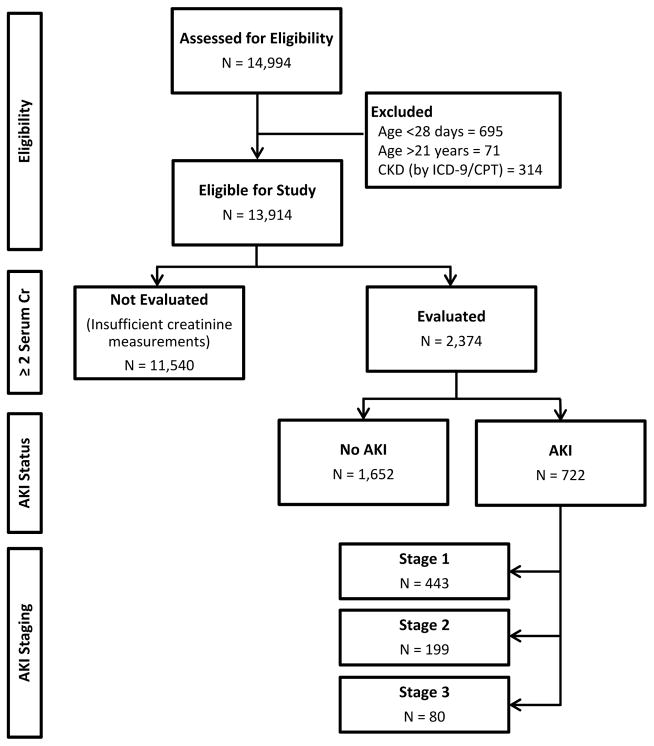
Setting & participants: 13,914 noncritical admissions during 2011 and 2012 at our tertiary referral pediatric hospital were evaluated. Patients younger than 28 days or older than 21 years of age or with chronic kidney disease (CKD) were excluded. Admissions with 2 or more serum creatinine measurements were evaluated.
Factors: Demographic features, laboratory measurements, medication exposures, and length of stay.
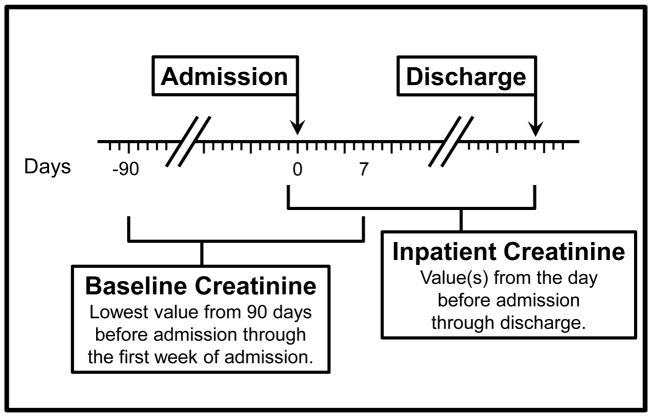
Outcome: AKI defined as increased serum creatinine level in accordance with KDIGO (Kidney Disease: Improving Global Outcomes) criteria. Based on time of admission, time interval requirements were met in 97% of cases, but KDIGO time window criteria were not strictly enforced to allow implementation using clinically obtained data.
Results: 2 or more creatinine measurements (one baseline before or during admission and a second during admission) in 2,374 of 13,914 (17%) patients allowed for AKI evaluation. A serum creatinine difference ≥0.3mg/dL or ≥1.5 times baseline was seen in 722 of 2,374 (30%) patients. A minimum of 5% of all noncritical inpatients without CKD in pediatric wards have an episode of AKI during routine hospital admission.
Limitations: Urine output, glomerular filtration rate, and time interval criteria for AKI were not applied secondary to study design and available data. The evaluated cohort was restricted to patients with 2 or more clinically obtained serum creatinine measurements, and baseline creatinine level may have been measured after the AKI episode.
Conclusions: AKI occurs in at least 5% of all noncritically ill hospitalized children, adolescents, and young adults without known CKD. Physicians should increase their awareness of AKI and improve surveillance strategies with serum creatinine measurements in this population so that exacerbating factors such as nephrotoxic medication exposures may be modified as indicated.
Keywords: Acute kidney injury (AKI); KDIGO AKI criteria; acute renal failure (ARF); children, adolescents, young adults, electronic medical records (EMRs); incidence; inpatient pediatrics; medication exposure; nephrotoxicity; serum creatinine.
Copyright © 2016 National Kidney Foundation, Inc. Published by Elsevier Inc. All rights reserved.
Figures
References
-
- Ricci Z, Cruz DN, Ronco C. Classification and staging of acute kidney injury: beyond the RIFLE and AKIN criteria. Nat Rev Nephrol. 2011 Apr;7(4):201–208. - PubMed
-
- Chertow GM, Burdick E, Honour M, Bonventre JV, Bates DW. Acute kidney injury, mortality, length of stay, and costs in hospitalized patients. J Am Soc Nephrol. 2005 Nov;16(11):3365–3370. - PubMed
-
- Akcan-Arikan A, Zappitelli M, Loftis LL, Washburn KK, Jefferson LS, Goldstein SL. Modified RIFLE criteria in critically ill children with acute kidney injury. Kidney Int. 2007 May;71(10):1028–1035. - PubMed
-
- Askenazi DJ, Feig DI, Graham NM, Hui-Stickle S, Goldstein SL. 3–5 year longitudinal follow-up of pediatric patients after acute renal failure. Kidney Int. 2006 Jan;69(1):184–189. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
