

Fluid administration and morbidity in transhiatal esophagectomy
- PMID: 26319974
- PMCID: PMC4914131
- DOI: 10.1016/j.jss.2015.07.021
Fluid administration and morbidity in transhiatal esophagectomy
Abstract
Background: Esophagectomy is associated with significant morbidity. Optimizing perioperative fluid administration is one potential strategy to mitigate morbidity. We sought to investigate the relationship of intraoperative fluid (IOF) administration to outcomes in patients undergoing transhiatal esophagectomy with particular attention to malnourished patients, who may be more susceptible to the effects of fluid overload.
Material and methods: Patients who underwent transhiatal esophagectomy from 2000-2013 were identified from a retrospective database. IOF rates (mL/kg/hr) were determined and their relationship to outcomes compared. To examine the impact of malnutrition, we stratified patients based on median preoperative serum albumin and compared outcomes.
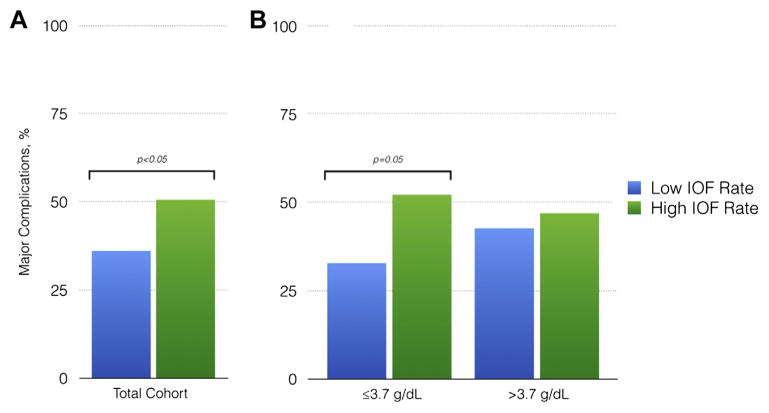
Results and discussion: 211 patients comprised the cohort. 74% of patients underwent esophagectomy for esophageal adenocarcinoma. Linear regression analyses were performed comparing independent perioperative variables to four outcomes variables: length of stay, complications per patient, major complications, and Clavien-Dindo classification. IOF rate was significantly associated with three of four outcomes on univariate analysis. Significantly more patients with a preoperative albumin level ≤3.7 g/dL who received more than the median IOF rate experienced more severe complications.
Conclusions: Increased intraoperative fluid administration is associated with perioperative morbidity in patients undergoing transhiatal esophagectomy. Patients with lower preoperative albumin levels may be particularly sensitive to the effects of volume overload.
Keywords: Fluids; Morbidity; Transhiatal esophagectomy.
Copyright © 2016 Elsevier Inc. All rights reserved.
Figures
References
-
- Bailey SH, Bull DA, Harpole DH, et al. Outcomes after esophagectomy: a ten-year prospective cohort. Ann Thorac Surg. 2003;75:217. discussion 222. - PubMed
-
- Ferguson MK, Celauro AD, Prachand V. Prediction of major pulmonary complications after esophagectomy. Ann Thorac Surg. 2011;91:1494. discussion 1500–1491. - PubMed
-
- Markar SR, Schmidt H, Kunz S, et al. Evolution of standardized clinical pathways: refining multidisciplinary care and process to improve outcomes of the surgical treatment of esophageal cancer. J Gastrointest Surg. 2014;18:1238. - PubMed
Publication types
MeSH terms
Supplementary concepts
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
