

Laparoscopic decompression as treatment for median arcuate ligament syndrome
- PMID: 26320770
- PMCID: PMC5126249
- DOI: 10.1308/rcsann.2015.0025
Laparoscopic decompression as treatment for median arcuate ligament syndrome
Abstract
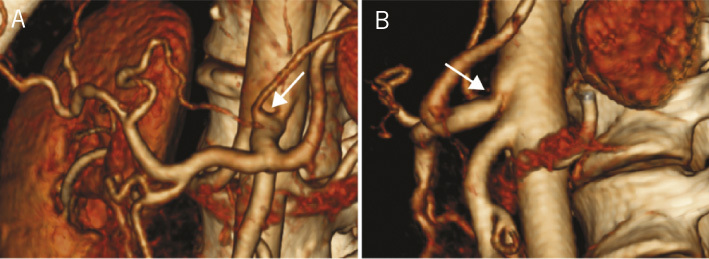
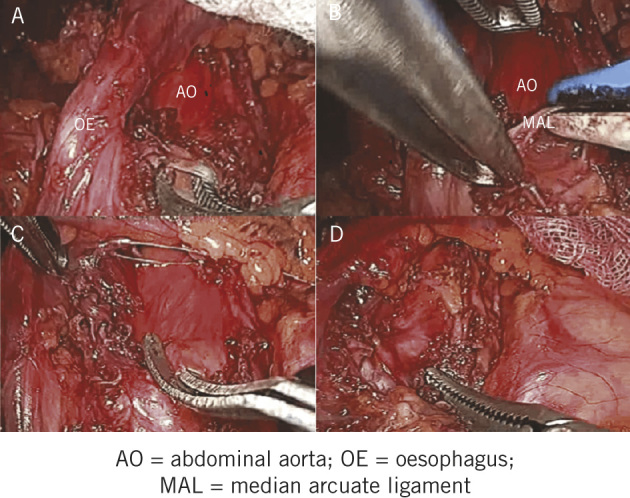
Median arcuate ligament syndrome (MALS) is a rare disorder due to coeliac trunk compression by the median arcuate ligament, resulting in coeliac artery stenosis characterised by chronic, recurrent abdominal pain. Patients with MALS are often middle-aged females presenting with a triad of postprandial epigastric pain, weight loss and abdominal bruit. It is a diagnosis of exclusion and confirmed by computed tomography or magnetic resonance imaging. Laparoscopic or open surgical decompression are the only treatment options in MALS. We present two cases of MALS treated by laparoscopic decompression as well as a literature review on this treatment.
Keywords: Coeliac artery compression syndrome; Dunbar syndrome; Laparoscopic decompression; Median arcuate ligament syndrome.
Figures

Similar articles
-
[Laparoscopic Division of the Arcuate Ligament: Treatment of the Coeliac Artery Compression Syndrome].Zentralbl Chir. 2016 Oct;141(5):505-508. doi: 10.1055/s-0042-102534. Epub 2016 Jun 13. Zentralbl Chir. 2016. PMID: 27294602 German.
-
Median arcuate ligament syndrome in the pediatric population.J Pediatr Surg. 2013 Nov;48(11):2261-70. doi: 10.1016/j.jpedsurg.2013.03.003. J Pediatr Surg. 2013. PMID: 24210197 Free PMC article.
-
Median Arcuate Ligament Syndrome-Review of This Rare Disease.JAMA Surg. 2016 May 1;151(5):471-7. doi: 10.1001/jamasurg.2016.0002. JAMA Surg. 2016. PMID: 26934394 Review.
-
Treatment of median arcuate ligament syndrome via traditional and robotic techniques.Hawaii J Med Public Health. 2013 Aug;72(8):279-81. Hawaii J Med Public Health. 2013. PMID: 24349891 Free PMC article.
-
Median Arcuate Ligament Syndrome - Literature Review and Case Report.Rev Port Cir Cardiotorac Vasc. 2017 Jul-Dec;24(3-4):111. Rev Port Cir Cardiotorac Vasc. 2017. PMID: 29701344 Review.
Cited by
-
An Atypical Presentation of Median Arcuate Ligament Syndrome.Cureus. 2020 Mar 16;12(3):e7289. doi: 10.7759/cureus.7289. Cureus. 2020. PMID: 32300508 Free PMC article.
-
Hybrid (laparoscopy + stent) treatment of celiac trunk compression syndrome (Dunbar syndrome, median arcuate ligament syndrome (MALS)).Wideochir Inne Tech Maloinwazyjne. 2016;11(4):236-239. doi: 10.5114/wiitm.2016.64070. Epub 2016 Dec 2. Wideochir Inne Tech Maloinwazyjne. 2016. PMID: 28194242 Free PMC article.
-
Robotic approach to treat Median Arcuate Ligament syndrome: a case report.J Surg Case Rep. 2020 May 18;2020(5):rjaa088. doi: 10.1093/jscr/rjaa088. eCollection 2020 May. J Surg Case Rep. 2020. PMID: 32440331 Free PMC article.
-
An unusual cause of epigastric pain and diaphoresis.Heliyon. 2020 Feb 28;6(2):e03509. doi: 10.1016/j.heliyon.2020.e03509. eCollection 2020 Feb. Heliyon. 2020. PMID: 32140607 Free PMC article.
-
Overview of Median Arcuate Ligament Syndrome: A Narrative Review.Cureus. 2023 Oct 8;15(10):e46675. doi: 10.7759/cureus.46675. eCollection 2023 Oct. Cureus. 2023. PMID: 37942382 Free PMC article. Review.
References
-
- Harjola PT. A rare obstruction of the coeliac artery. Report of a case . Ann Chir Gynaecol Fenn 1963. ; : 547–550. - PubMed
-
- Dunbar JD, Molnar W, Beman FF, Marable SA. Compression of the celiac trunk and abdominal angina . Am J Roentgenol Radium Ther Nucl Med 1965. ; : 731–744. - PubMed
-
- Kazan V, Qu W, Al-Natour M et al. . Celiac artery compression syndrome: a radiological finding without clinical symptoms? Vascular 2013 March 18. [Epub ahead of print.] - PubMed
-
- Faries PL, Narula A, Veith FJ. et al. . The use of gastric tonometry in the assessment of celiac artery compression syndrome . Ann Vasc Surg 2000. ; : 20–23. - PubMed
-
- Roseborough GS. Laparoscopic management of celiac artery compression syndrome . J Vasc Surg 2009. ; : 124–133. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources