

The consequence of biologic graft processing on blood interface biocompatibility and mechanics
- PMID: 26322140
- PMCID: PMC4548972
- DOI: 10.1007/s13239-015-0221-2
The consequence of biologic graft processing on blood interface biocompatibility and mechanics
Abstract
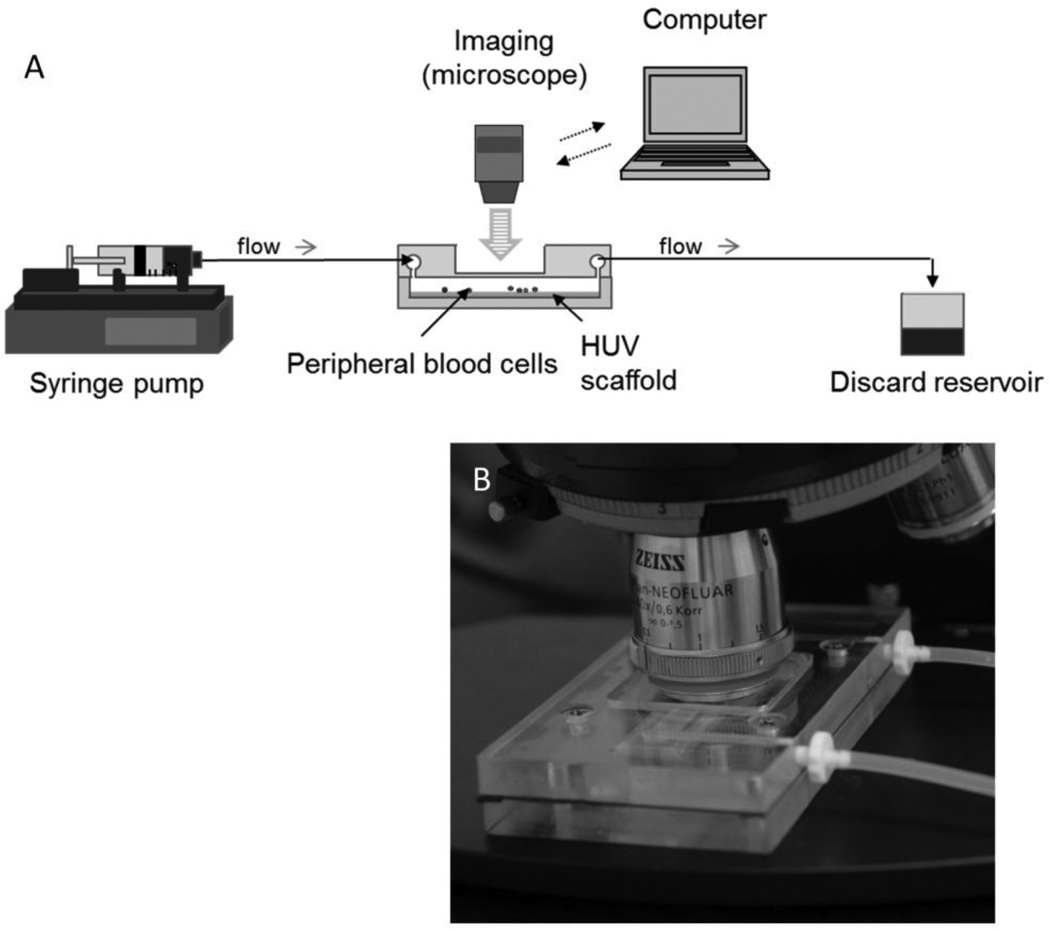
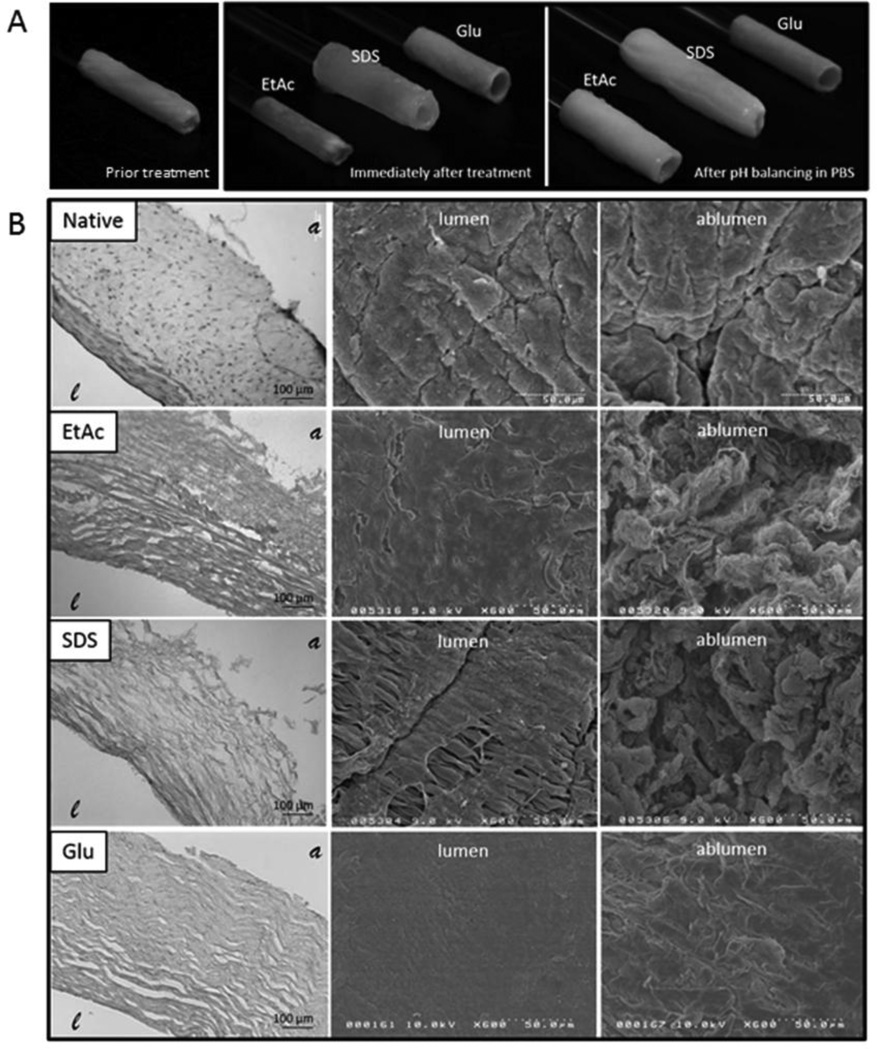
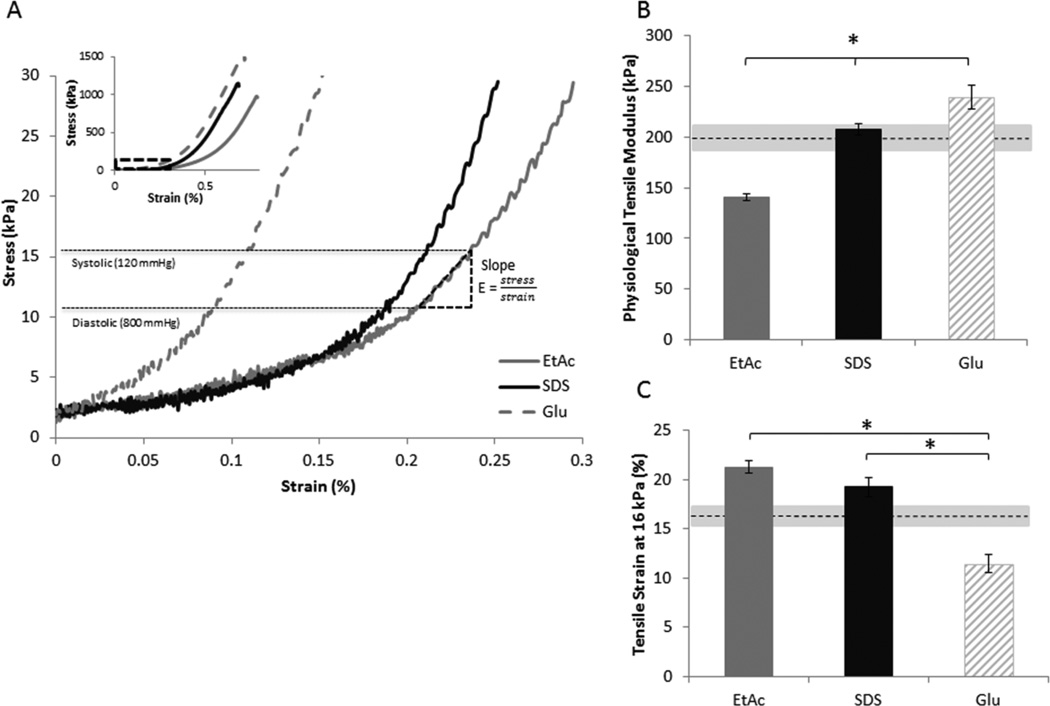
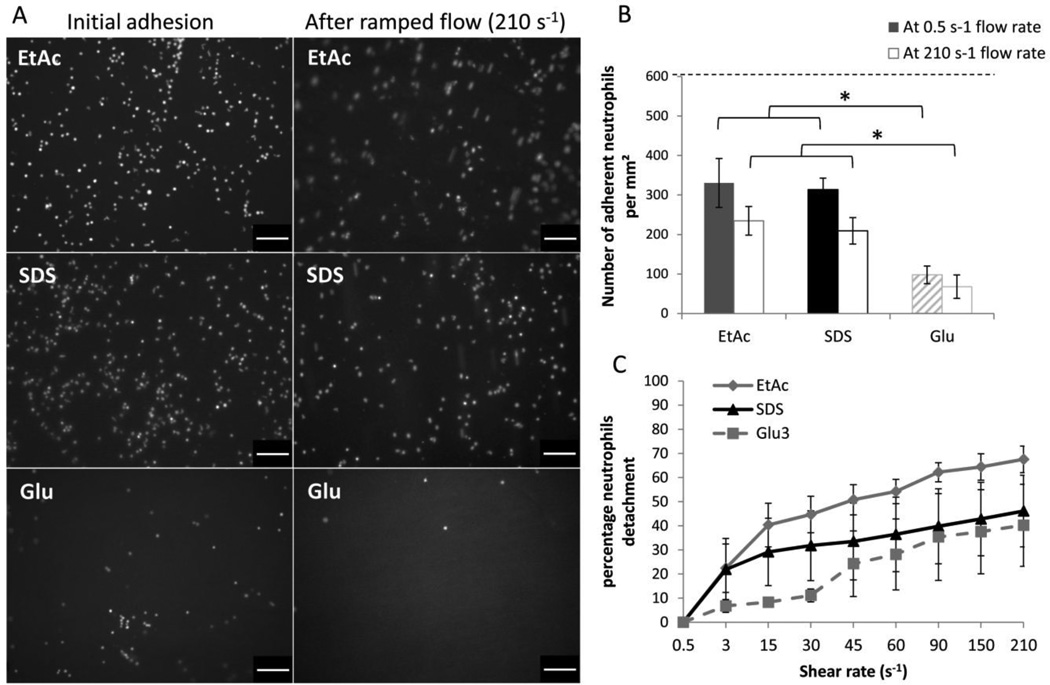
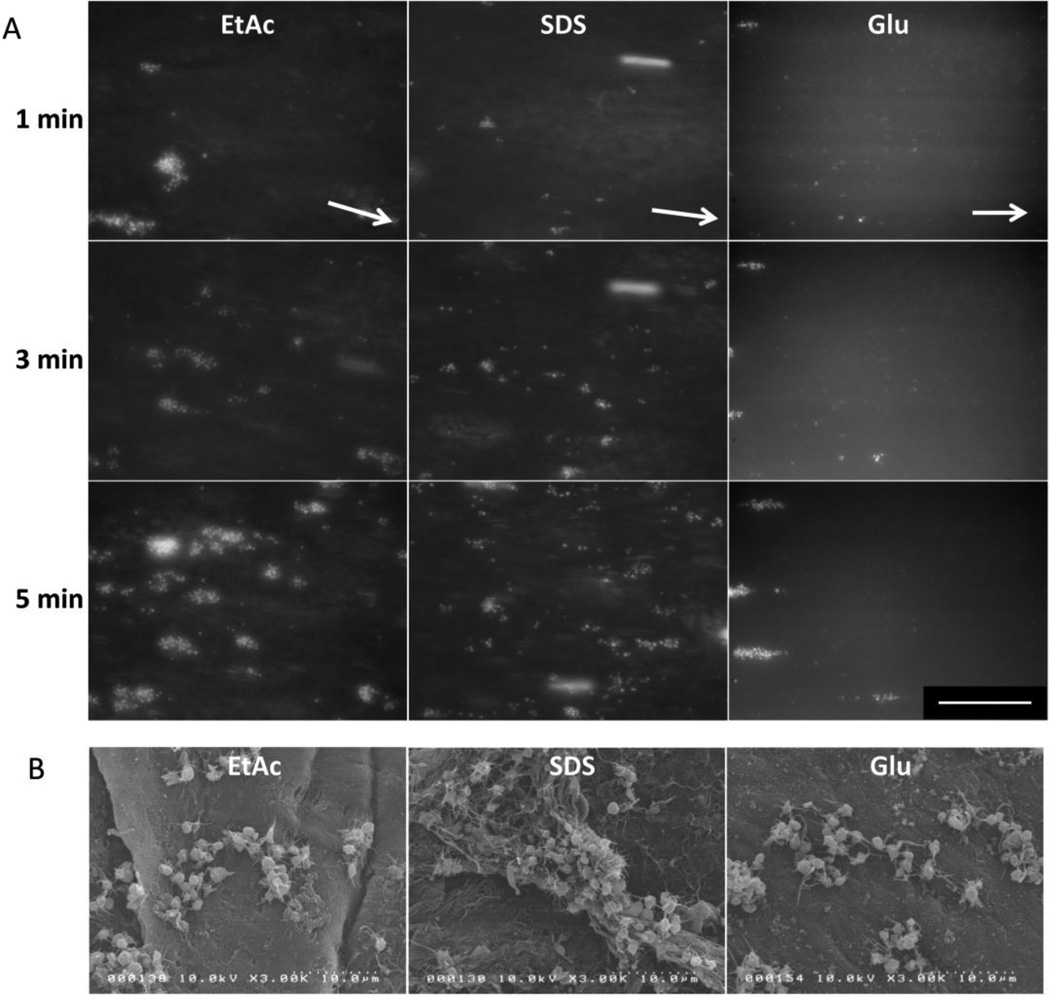
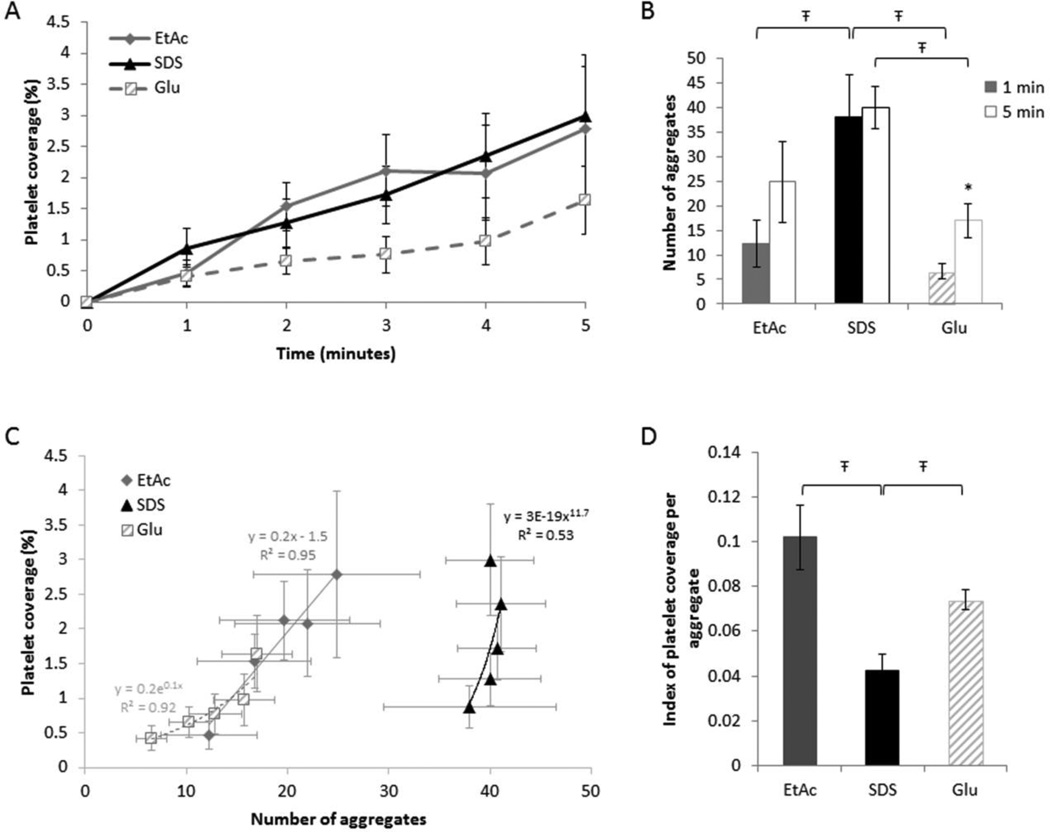
Processing ex vivo derived tissues to reduce immunogenicity is an effective approach to create biologically complex materials for vascular reconstruction. Due to the sensitivity of small diameter vascular grafts to occlusive events, the effect of graft processing on critical parameters for graft patency, such as peripheral cell adhesion and wall mechanics, requires detailed analysis. Isolated human umbilical vein sections were used as model allogenic vascular scaffolds that were processed with either: 1. sodium dodecyl sulfate (SDS), 2. ethanol/acetone (EtAc), or 3. glutaraldehyde (Glu). Changes in material mechanics were assessed via uniaxial tensile testing. Peripheral cell adhesion to the opaque grafting material was evaluated using an innovative flow chamber that allows direct observation of the blood-graft interface under physiological shear conditions. All treatments modified the grafts tensile strain and stiffness properties, with physiological modulus values decreasing from Glu 240±12 kPa to SDS 210±6 kPa and EtAc 140±3 kPa, P<.001. Relative to glutaraldehyde treatments, neutrophil adhesion to the decellularized grafts increased, with no statistical difference observed between SDS or EtAc treatments. Early platelet adhesion (% surface coverage) showed no statistical difference between the three treatments; however, quantification of platelet aggregates was significantly higher on SDS scaffolds compared to EtAc or Glu. Tissue processing strategies applied to the umbilical vein scaffold were shown to modify structural mechanics and cell adhesion properties, with the EtAc treatment reducing thrombotic events relative to SDS treated samples. This approach allows time and cost effective prescreening of clinically relevant grafting materials to assess initial cell reactivity.
Keywords: biocompatibility; biomaterial; decellularization; flow chamber; human umbilical vein; thrombosis; vascular tissue engineering.
Figures
References
-
- Garrett HE, Dennis EW, DeBakey ME. Aortocoronary bypass with saphenous vein graft. Seven-year follow-up. JAMA. 1973;223:792–794. - PubMed
-
- Gibson KD, Gillen DL, Caps MT, Kohler TR, Sherrard DJ, Stehman-Breen CO. Vascular access survival and incidence of revisions: A comparison of prosthetic grafts, simple autogenous fistulas, and venous transposition fistulas from the United States Renal Data System Dialysis Morbidity and Mortality Study. Journal of Vascular Surgery. 2001;34:694–700. - PubMed
-
- Johnson WC, Lee KK. A comparative evaluation of polytetrafluoroethylene, umbilical vein, and saphenous vein bypass grafts for femoral-popliteal above-knee revascularization: a prospective randomized Department of Veterans Affairs cooperative study. J. Vasc. Surg. 2000;32:268–277. - PubMed
-
- Dardik H, Wengerter K, Qin F, Pangilinan A, Silvestri F, Wolodiger F, et al. Comparative decades of experience with glutaraldehyde-tanned human umbilical cord vein graft for lower limb revascularization: An analysis of 1275 cases. Journal of Vascular Surgery. 2002;35:64–71. - PubMed
-
- Dardik A, Dardik H. Umbilical Vein Grafts for Lower Limb Revascularization. In: Bhattacharya N, Stubblefield P, editors. Regenerative Medicine Using Pregnancy-Specific Biological Substances [Internet] Springer London: 2011. [cited 2014 Oct 20]. pp. 189–198. Available from: http://link.springer.com/chapter/10.1007/978-1-84882-718-9_19. - DOI
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
