

Early repolarization syndrome: A cause of sudden cardiac death
- PMID: 26322186
- PMCID: PMC4549780
- DOI: 10.4330/wjc.v7.i8.466
Early repolarization syndrome: A cause of sudden cardiac death
Abstract
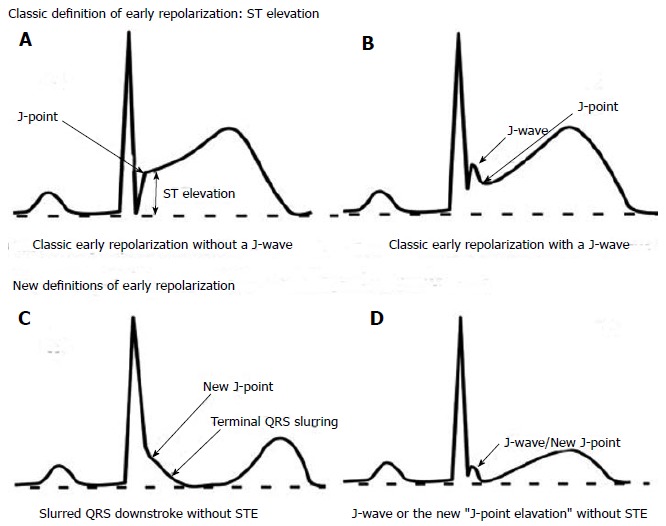
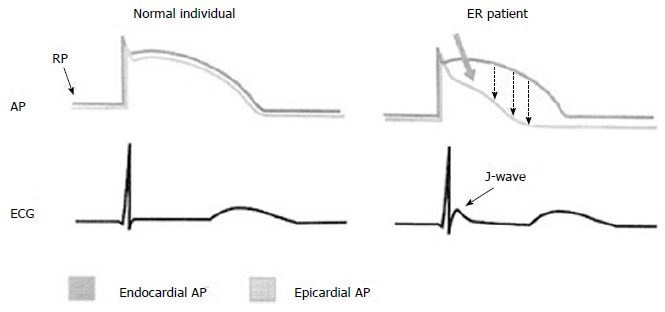
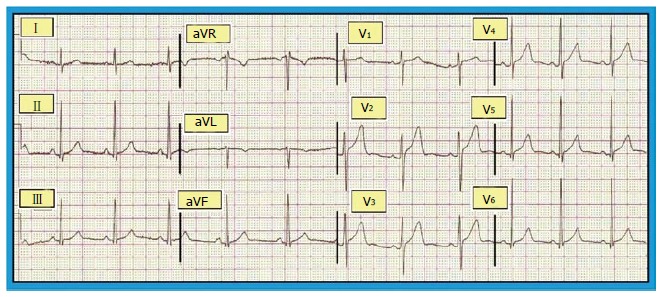
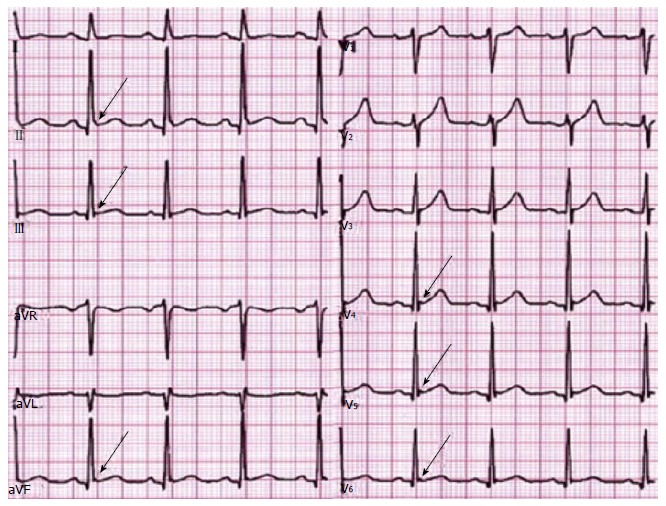
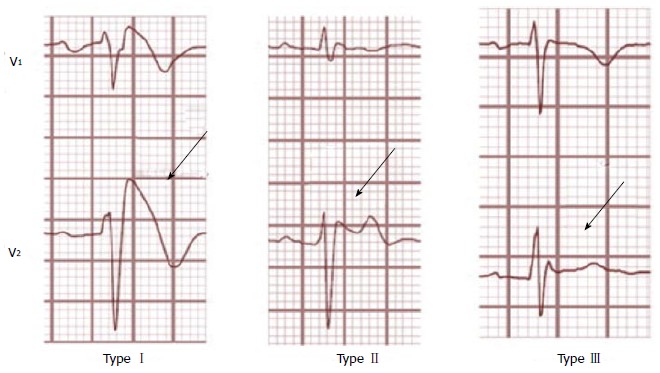
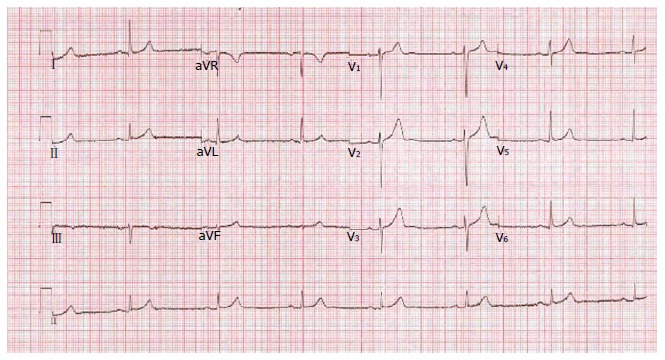
Early repolarization syndrome (ERS), demonstrated as J-point elevation on an electrocardiograph, was formerly thought to be a benign entity, but the recent studies have demonstrated that it can be linked to a considerable risk of life - threatening arrhythmias and sudden cardiac death (SCD). Early repolarization characteristics associated with SCD include high - amplitude J-point elevation, horizontal and/or downslopping ST segments, and inferior and/or lateral leads location. The prevalence of ERS varies between 3% and 24%, depending on age, sex and J-point elevation (0.05 mV vs 0.1 mV) being the main determinants. ERS patients are sporadic and they are at a higher risk of having recurrent cardiac events. Implantable cardioverter-defibrillator implantation and isoproterenol are the suggested therapies in this set of patients. On the other hand, asymptomatic patients with ERS are common and have a better prognosis. The risk stratification in asymptomatic patients with ERS still remains a grey area. This review provides an outline of the up-to-date evidence associated with ERS and the risk of life - threatening arrhythmias. Further prospective studies are required to elucidate the mechanisms of ventricular arrhythmogenesis in patients with ERS.
Keywords: Early repolarization; Early repolarization syndrome; J-wave; Sudden cardiac death.
Figures
References
-
- Brugada J, Brugada R, Brugada P. Right bundle-branch block and ST-segment elevation in leads V1 through V3: a marker for sudden death in patients without demonstrable structural heart disease. Circulation. 1998;97:457–460. - PubMed
-
- Zipes DP, Wellens HJ. Sudden cardiac death. Circulation. 1998;98:2334–2351. - PubMed
-
- Moss AJ, Schwartz PJ, Crampton RS, Locati E, Carleen E. The long QT syndrome: a prospective international study. Circulation. 1985;71:17–21. - PubMed
-
- Gaita F, Giustetto C, Bianchi F, Wolpert C, Schimpf R, Riccardi R, Grossi S, Richiardi E, Borggrefe M. Short QT Syndrome: a familial cause of sudden death. Circulation. 2003;108:965–970. - PubMed
-
- Corrado D, Basso C, Thiene G. Sudden cardiac death in young people with apparently normal heart. Cardiovasc Res. 2001;50:399–408. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
