

HIV-1 Drug Resistance and Second-Line Treatment in Children Randomized to Switch at Low Versus Higher RNA Thresholds
- PMID: 26322666
- PMCID: PMC4556171
- DOI: 10.1097/QAI.0000000000000671
HIV-1 Drug Resistance and Second-Line Treatment in Children Randomized to Switch at Low Versus Higher RNA Thresholds
Abstract
Background: The PENPACT-1 trial compared virologic thresholds to determine when to switch to second-line antiretroviral therapy (ART). Using PENPACT-1 data, we aimed to describe HIV-1 drug resistance accumulation on first-line ART by virologic threshold.
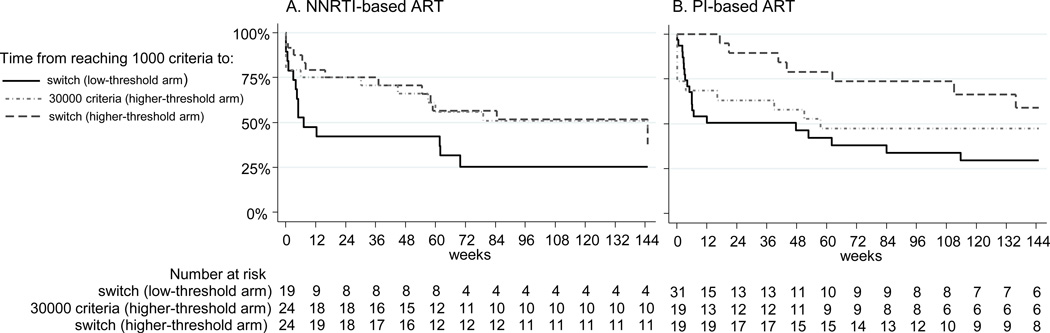
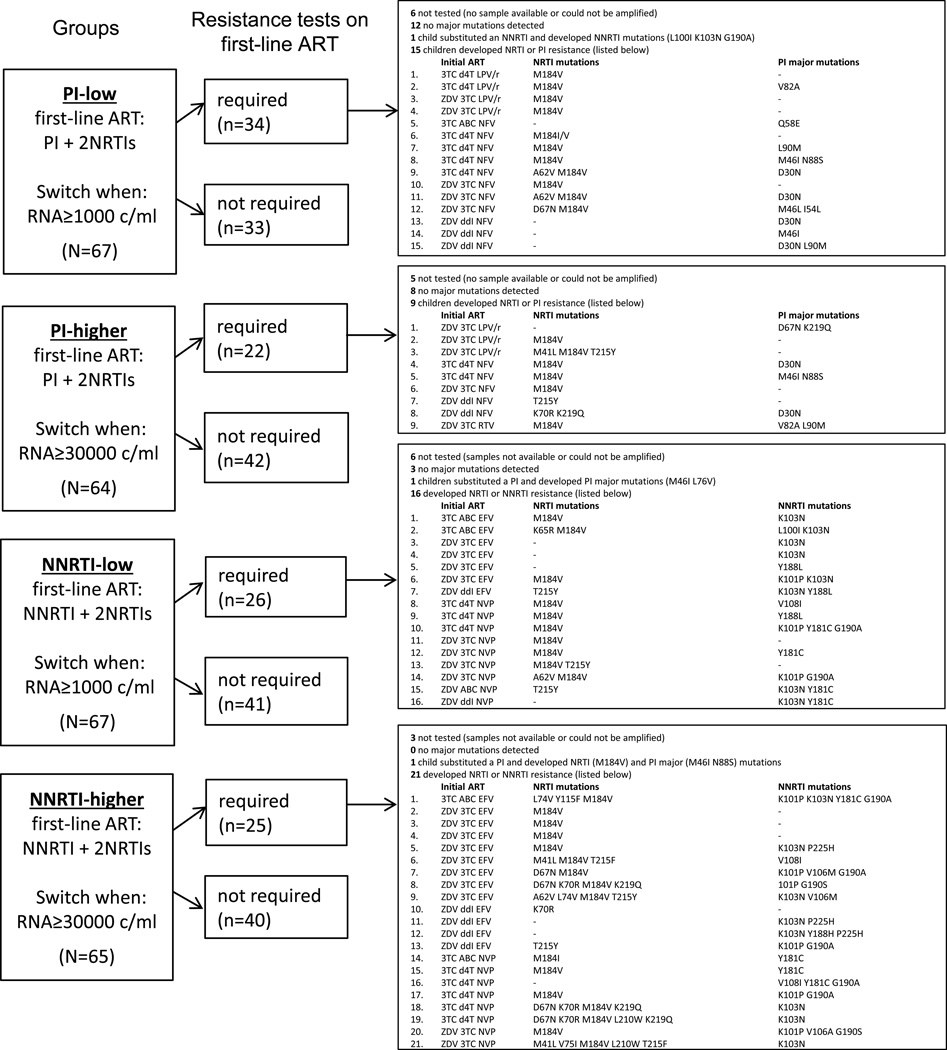
Methods: PENPACT-1 had a 2 × 2 factorial design, randomizing HIV-infected children to start protease inhibitor (PI) versus nonnucleoside reverse transcriptase inhibitor (NNRTI)-based ART, and switch at a 1000 copies/mL versus 30,000 copies/mL threshold. Switch criteria were not achieving the threshold by week 24, confirmed rebound above the threshold thereafter, or Center for Disease Control and Prevention stage C event. Resistance tests were performed on samples ≥1000 copies/mL before switch, resuppression, and at 4-years/trial end.
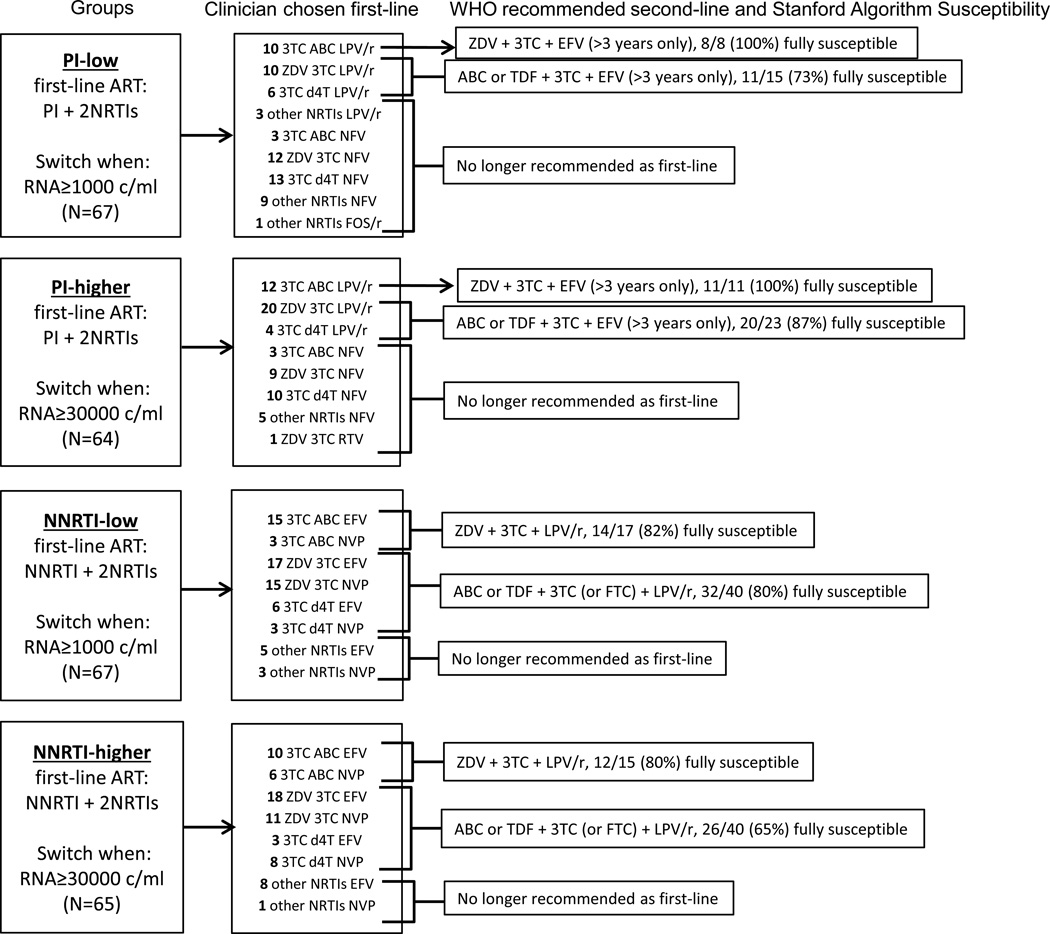
Results: Sixty-seven children started PI-based ART and were randomized to switch at 1000 copies/mL (PI-1000), 64 PIs and 30,000 copies/mL (PI-30,000), 67 NNRTIs and 1000 copies/mL (NNRTI-1000), and 65 NNRTI and 30,000 copies/mL (NNRTI-30,000). Ninety-four (36%) children reached the 1000 copies/mL switch criteria during 5-year follow-up. In 30,000 copies/mL threshold arms, median time from 1000 to 30,000 copies/mL switch criteria was 58 (PI) versus 80 (NNRTI) weeks (P = 0.81). In NNRTI-30,000, more nucleoside reverse transcriptase inhibitor (NRTI) resistance mutations accumulated than other groups. NNRTI mutations were selected before switching at 1000 copies/mL (23% NNRTI-1000, 27% NNRTI-30,000). Sixty-two children started abacavir + lamivudine, 166 lamivudine + zidovudine or stavudine, and 35 other NRTIs. The abacavir + lamivudine group acquired fewest NRTI mutations. Of 60 switched to second-line, 79% PI-1000, 63% PI-30,000, 64% NNRTI-1000, and 100% NNRTI-30,000 were <400 copies/mL 24 weeks later.
Conclusions: Children on first-line NNRTI-based ART who were randomized to switch at a higher virologic threshold developed the most resistance, yet resuppressed on second-line. An abacavir + lamivudine NRTI combination seemed protective against development of NRTI resistance.
Conflict of interest statement
Figures
References
-
- World Health Organisation. Consolidated Guidelines on the use of Antiretroviral Drugs for Treating and Preventing HIV Infection; Recommendations for a Public Health Approach. 2013 Jun - PubMed
-
- Panel on Antiretroviral Therapy and Medical Management of HIV-Infected Children. Guidelines for the Use of Antiretroviral Agents in Pediatric HIV Infection. Available at: http://aidsinfo.nih.gov/guidelines.
-
- PENTA Steering Committee. PENTA 2009 Guidelines for the use of antiretroviral therapy in paediatric HIV-1 infection. HIV Med. 2009;10:591–613. - PubMed
-
- PENPACT-1 (PENTA 9/PACTG 390) Study Team. Babiker A, Castro nee Green H, Compagnucci A, Fiscus S, Giaquinto C, Gibb DM, Harper L, Harrison L, Hughes M, McKinney R, Melvin A, Mofenson L, Saidi Y, Smith ME, Tudor-Williams G, Walker AS. First-line antiretroviral therapy with a protease inhibitor versus non-nucleoside reverse transcriptase inhibitor and switch at higher versus low viral load in HIV-infected children: an open-label, randomised phase 2/3 trial. Lancet Infect Dis. 2011;11(4):273–283. - PMC - PubMed
-
- Johnson VA, Brun-Vezinet, Clotet B, et al. Update of the drug resistance mutations in HIV-1: December 2009. Top HIV Med. 2009;17:138–145. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- UM1AI106716/AI/NIAID NIH HHS/United States
- MC_UU_12023/16/MRC_/Medical Research Council/United Kingdom
- UM1 AI068632/AI/NIAID NIH HHS/United States
- UM1 AI069415/AI/NIAID NIH HHS/United States
- M01 RR016587/RR/NCRR NIH HHS/United States
- MC_UU_12023/26/MRC_/Medical Research Council/United Kingdom
- MC_UU_12023/23/MRC_/Medical Research Council/United Kingdom
- UM1 AI068616/AI/NIAID NIH HHS/United States
- UM1AI068616/AI/NIAID NIH HHS/United States
- UM1 AI106716/AI/NIAID NIH HHS/United States
- UM1AI068632/AI/NIAID NIH HHS/United States
- MC_U122886352/MRC_/Medical Research Council/United Kingdom
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
