

Increased Fracture Incidence in Middle-Aged HIV-Infected and HIV-Uninfected Women: Updated Results From the Women's Interagency HIV Study
- PMID: 26322667
- PMCID: PMC4557627
- DOI: 10.1097/QAI.0000000000000674
Increased Fracture Incidence in Middle-Aged HIV-Infected and HIV-Uninfected Women: Updated Results From the Women's Interagency HIV Study
Abstract
Background: We previously reported that fracture incidence rates did not differ by HIV status among predominantly premenopausal Women's Interagency HIV Study participants. We now conduct a follow-up study with 5 additional observation years to further characterize fracture risk associated with HIV infection in women as they age.
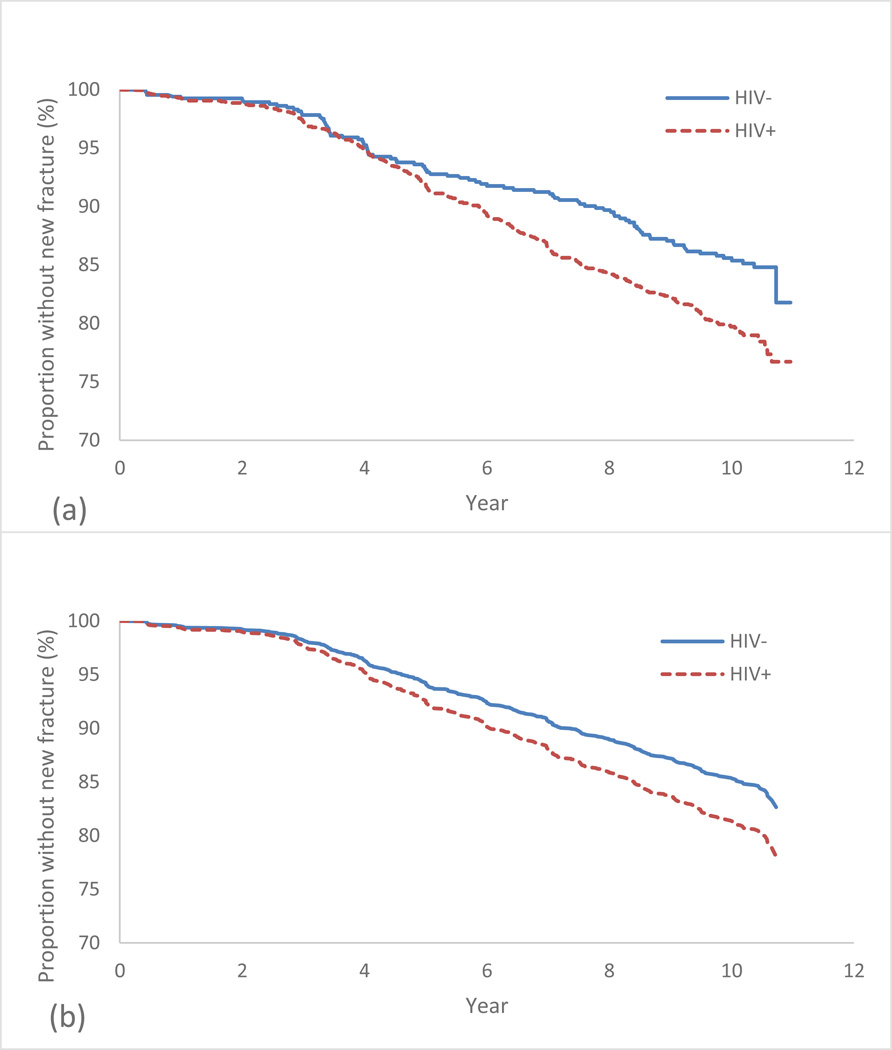
Methods: We measured time to first new fracture at any site in 2375 (1713 HIV-infected and 662 HIV-uninfected) Women's Interagency HIV Study participants, with median 10-year follow-up. Fractures were self-reported semiannually. Proportional hazards models assessed predictors of incident fracture.
Results: At index visit, HIV-infected women were older [median age of 40 years (IQR: 34-46) vs. 35 (27-43), P < 0.0001] and more likely to be postmenopausal, hepatitis C virus infected, and weigh less than HIV-uninfected women. Among HIV-infected women, mean CD4 count was 480 cells per microliter and 63% were taking highly active antiretroviral therapy. Unadjusted incidence rates of any fracture were higher in HIV-infected than in HIV-uninfected women [2.19/100 person-years (py) vs. 1.54/100 py, P = 0.002]. In multivariate models, HIV status, older age, white (vs. black) race, prior fracture, history of cocaine use, and history of injection drug use were significant predictors of incident fracture. Among HIV-infected women, age, white race, prior fracture, smoking, and prior AIDS were predictors of new fracture.
Conclusions: Middle-aged HIV-infected women had a higher adjusted fracture rate than HIV-uninfected women. Cocaine use and injection drug use were also associated with a greater risk of incident fracture. Further research is needed to understand whether the risk of fracture associated with cocaine use relates to increased rate of falls or direct effects on bone metabolism.
Conflict of interest statement
Figures
Similar articles
-
Fracture incidence in HIV-infected women: results from the Women's Interagency HIV Study.AIDS. 2010 Nov 13;24(17):2679-86. doi: 10.1097/QAD.0b013e32833f6294. AIDS. 2010. PMID: 20859192 Free PMC article.
-
Increased rates of bone fracture among HIV-infected persons in the HIV Outpatient Study (HOPS) compared with the US general population, 2000-2006.Clin Infect Dis. 2011 Apr 15;52(8):1061-8. doi: 10.1093/cid/ciq242. Epub 2011 Mar 10. Clin Infect Dis. 2011. PMID: 21398272
-
Hormone therapy and fractures in postmenopausal women.AIDS. 2022 Oct 1;36(12):1683-1688. doi: 10.1097/QAD.0000000000003292. Epub 2022 Jun 22. AIDS. 2022. PMID: 35730385 Free PMC article.
-
More than osteoporosis: age-specific issues in bone health.Curr Opin HIV AIDS. 2016 May;11(3):343-50. doi: 10.1097/COH.0000000000000258. Curr Opin HIV AIDS. 2016. PMID: 26882460 Free PMC article. Review.
-
HIV and Aging Research in Women: An Overview.Curr HIV/AIDS Rep. 2016 Dec;13(6):383-391. doi: 10.1007/s11904-016-0338-4. Curr HIV/AIDS Rep. 2016. PMID: 27771876 Review.
Cited by
-
Treatment of Human Immunodeficiency Virus Infection With Tenofovir Disoproxil Fumarate-Containing Antiretrovirals Maintains Low Bone Formation Rate, But Increases Osteoid Volume on Bone Histomorphometry.J Bone Miner Res. 2019 Sep;34(9):1574-1584. doi: 10.1002/jbmr.3751. Epub 2019 Jul 3. J Bone Miner Res. 2019. PMID: 31269294 Free PMC article.
-
Relationships Between Physical Activity and Bone Density in People Living with HIV: Results from the SATURN-HIV Study.J Assoc Nurses AIDS Care. 2018 Jul-Aug;29(4):528-537. doi: 10.1016/j.jana.2018.03.004. Epub 2018 Mar 28. J Assoc Nurses AIDS Care. 2018. PMID: 29735237 Free PMC article. Clinical Trial.
-
Emphysema is associated with thoracic vertebral bone attenuation on chest CT scan in HIV-infected individuals.PLoS One. 2017 Apr 27;12(4):e0176719. doi: 10.1371/journal.pone.0176719. eCollection 2017. PLoS One. 2017. PMID: 28448615 Free PMC article.
-
Lactobacillus rhamnosus GG attenuates tenofovir disoproxil fumarate-induced bone loss in male mice via gut-microbiota-dependent anti-inflammation.Ther Adv Chronic Dis. 2019 Jul 3;10:2040622319860653. doi: 10.1177/2040622319860653. eCollection 2019. Ther Adv Chronic Dis. 2019. PMID: 31321013 Free PMC article.
-
The Hidden Burden of Fractures in People Living With HIV.JBMR Plus. 2018 Jun 20;2(5):247-256. doi: 10.1002/jbm4.10055. eCollection 2018 Sep. JBMR Plus. 2018. PMID: 30283906 Free PMC article. Review.
References
-
- Brown TT, Qaqish RB. Antiretroviral therapy and the prevalence of osteopenia and osteoporosis: a meta-analytic review. AIDS. 2006;20:2165–2174. - PubMed
-
- Cazanave C, Dupon M, Lavignolle-Aurillac V, Barthe N, Lawson-Ayayi S, Mehsen N, et al. Reduced bone mineral density in HIV-infected patients: prevalence and associated factors. AIDS. 2008;22:395–402. - PubMed
-
- Mondy K, Yarasheski K, Powderly WG, Whyte M, Claxton S, DeMarco D, Hofman M, Tebas P. Longitudinal evolution of bone mineral density and bone markers in human immunodeficiency virus-infected individuals. Clin Infect Dis. 2003;36:482–490. - PubMed
-
- Bolland MJ, Grey AB, Gamble GD, Reid IR. CLINICAL Review: low body weight mediates the relationship between HIV infection and low bone mineral density: a meta-analysis. J Clin Endocrinol Metab. 2007 Dec;92(12):4522–4528. Epub 2007 Oct 9. - PubMed
Publication types
MeSH terms
Grants and funding
- UO1-HD-32632/HD/NICHD NIH HHS/United States
- U01 AI103397/AI/NIAID NIH HHS/United States
- UO1-AI-34994/AI/NIAID NIH HHS/United States
- U01-AI-103390/AI/NIAID NIH HHS/United States
- U01-AI-034994/AI/NIAID NIH HHS/United States
- U01-AI-103408/AI/NIAID NIH HHS/United States
- UO1-AI-34989/AI/NIAID NIH HHS/United States
- U01 AI031834/AI/NIAID NIH HHS/United States
- AI095089/AI/NIAID NIH HHS/United States
- UL1-TR000004/TR/NCATS NIH HHS/United States
- U01 AI035004/AI/NIAID NIH HHS/United States
- UL1-TR000454/TR/NCATS NIH HHS/United States
- U01-AI-034993/AI/NIAID NIH HHS/United States
- R01 AI095089/AI/NIAID NIH HHS/United States
- U01 AI034989/AI/NIAID NIH HHS/United States
- U01-AI-103401/AI/NIAID NIH HHS/United States
- U01-AI-035004/AI/NIAID NIH HHS/United States
- UO1-AI-35004/AI/NIAID NIH HHS/United States
- UO1-AI-34993/AI/NIAID NIH HHS/United States
- R03 DA029460/DA/NIDA NIH HHS/United States
- K23 AR061993/AR/NIAMS NIH HHS/United States
- U01 AI034994/AI/NIAID NIH HHS/United States
- UL1 TR000454/TR/NCATS NIH HHS/United States
- UL1 TR001073/TR/NCATS NIH HHS/United States
- U01-AI-103397/AI/NIAID NIH HHS/United States
- UL1 RR024131/RR/NCRR NIH HHS/United States
- U01 AI103401/AI/NIAID NIH HHS/United States
- K23AR06199301/AR/NIAMS NIH HHS/United States
- U01-AI-034989/AI/NIAID NIH HHS/United States
- U01-AI-042590/AI/NIAID NIH HHS/United States
- UO1-AI-42590/AI/NIAID NIH HHS/United States
- U01-HD-032632/HD/NICHD NIH HHS/United States
- U01 AI103390/AI/NIAID NIH HHS/United States
- D43 TW001035/TW/FIC NIH HHS/United States
- U01 AI034993/AI/NIAID NIH HHS/United States
- UO1-AI-31834/AI/NIAID NIH HHS/United States
- UL1 TR000004/TR/NCATS NIH HHS/United States
- U01 AI103408/AI/NIAID NIH HHS/United States
- U01-AI-031834/AI/NIAID NIH HHS/United States
- U01 HD032632/HD/NICHD NIH HHS/United States
- U01 AI042590/AI/NIAID NIH HHS/United States
