

Efficiency of Original versus Generic Intravenous Iron Formulations in Patients on Haemodialysis
- PMID: 26322790
- PMCID: PMC4555833
- DOI: 10.1371/journal.pone.0135967
Efficiency of Original versus Generic Intravenous Iron Formulations in Patients on Haemodialysis
Abstract
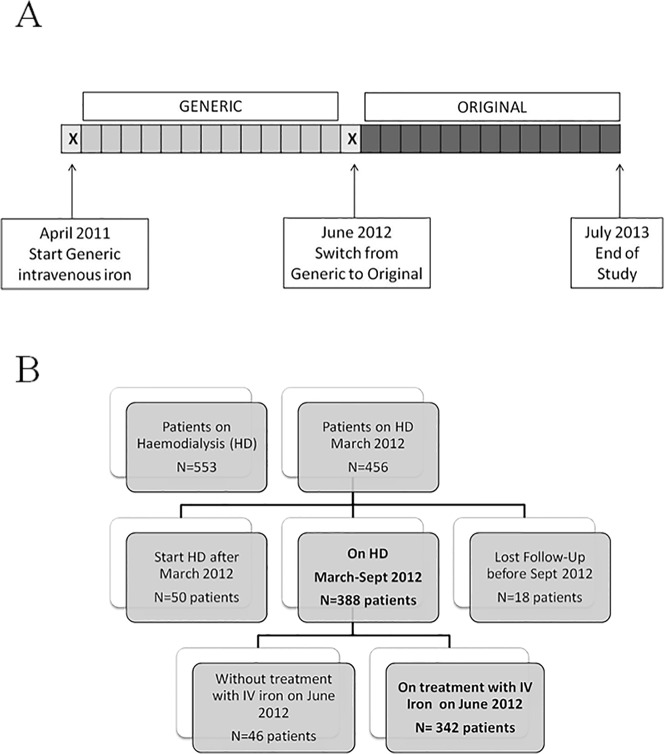
Aims: The appropriate use of intravenous (i.v.) iron is essential to minimise the requirements for erythropoiesis-stimulating agents (ESAs). The clinical efficacy of generic i.v. iron compared to the original formulation is controversial. We evaluated the changes that were induced after switching from a generic i.v. iron to an original formulation in a stable, prevalent haemodialysis (HD) population.
Methods: A total of 342 patients were included, and the follow-up period was 56 weeks for each formulation. Anaemia parameters and doses of ESA and i.v. iron were prospectively recorded before and after the switch from generic to original i.v. iron.
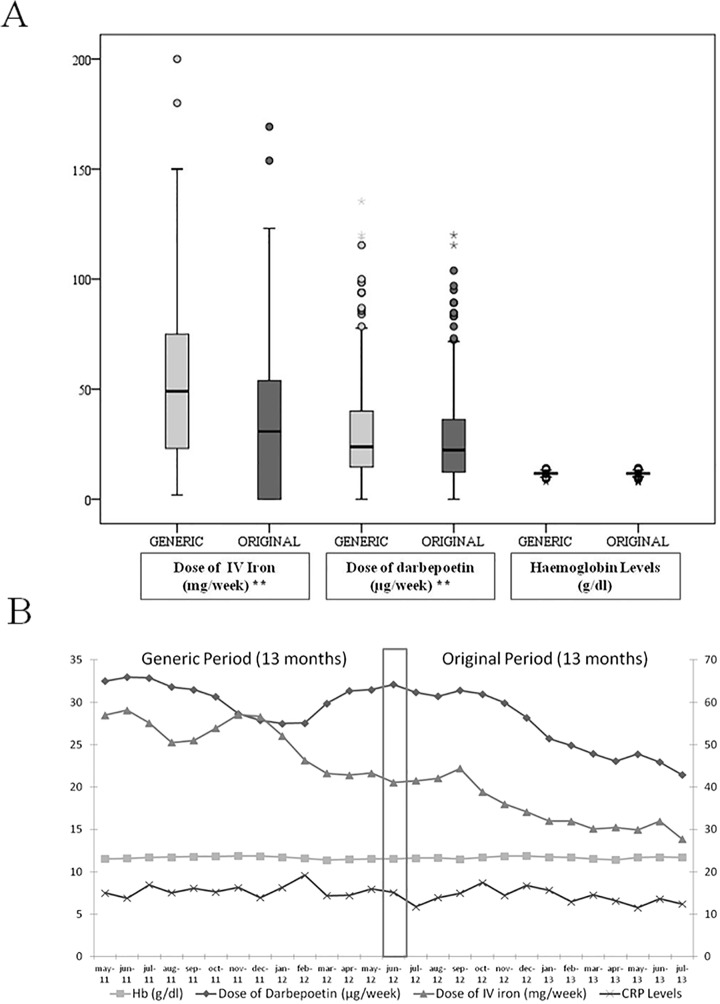
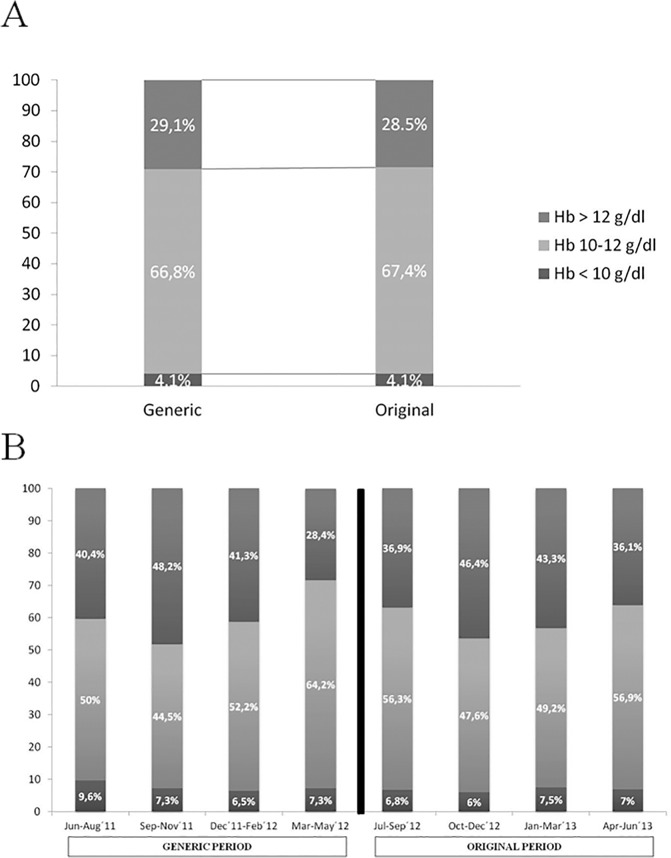
Results: To maintain the same haemoglobin (Hb) levels after switching from the generic to the original formulation, the requirements for i.v. iron doses were reduced by 34.3% (from 52.8±33.9 to 34.7±31.8 mg/week, p<0.001), and the ESA doses were also decreased by 12.5% (from 30.6±23.6 to 27±21 μg/week, p<0.001). The erythropoietin resistance index declined from 8.4±7.7 to 7.4±6.7 IU/kg/week/g/dl after the switch from the generic to the original drug (p = 0.001). After the switch, the transferrin saturation ratio (TSAT) and serum ferritin levels rose by 6.8% (p<0.001) and 12.4% (p = 0.001), respectively. The mortality rate was similar for both periods.
Conclusions: The iron and ESA requirements are lower with the original i.v. iron compared to the generic drug. In addition, the uses of the original formulation results in higher ferritin and TSAT levels despite the lower dose of i.v. iron. Further studies are necessary to analyse the adverse effects of higher i.v. iron dosages.
Conflict of interest statement
Figures

References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
