

Modeling the Health Effects of Expanding e-Cigarette Sales in the United States and United Kingdom: A Monte Carlo Analysis
- PMID: 26322924
- PMCID: PMC4594196
- DOI: 10.1001/jamainternmed.2015.4209
Modeling the Health Effects of Expanding e-Cigarette Sales in the United States and United Kingdom: A Monte Carlo Analysis
Abstract
Importance: The prevalence of electronic cigarette (e-cigarette) use is increasing. Population health effects will depend on cigarette smoking behaviors, levels of dual use with conventional cigarettes, and e-cigarette toxicity.
Objective: To evaluate potential health effects of various scenarios of increasing promotion and use of e-cigarettes.
Design, setting, and participants: A base case model was developed using data on actual cigarette and e-cigarette use patterns that quantifies transitions from an initial state of no cigarette or e-cigarette use to 1 of 5 final states: never use of cigarettes or e-cigarettes, cigarette use, e-cigarette use, dual use of cigarettes and e-cigarettes, or quit. Seven scenarios were created that cover a range of use patterns, depending on how the e-cigarette market might develop, as well as a range of possible long-term health effects of e-cigarette use. Scenarios for changes from the base case were evaluated using Monte Carlo simulations. Separate sets of base case model parameters were evaluated for the US and UK populations.
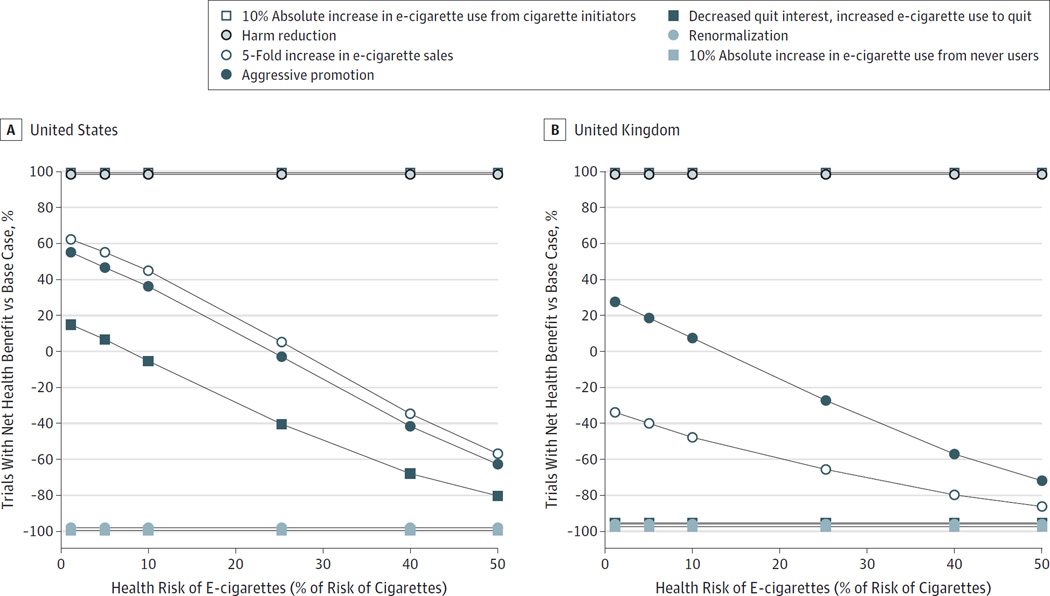
Main outcomes and measures: We assigned unitless health "costs" for each final state on a scale of 0 to 100. Population health "costs" were compared with the base case (status quo) assuming e-cigarette use health "costs" from 1% to 50% as dangerous as conventional cigarette use health costs.
Results: Compared with the base case, a harm reduction scenario in which e-cigarette use increases only among smokers who are interested in quitting with more quit attempts and no increased initiation of e-cigarette use among nonsmokers, and another scenario in which e-cigarettes are taken up only by youth who would have smoked conventional cigarettes, had population-level health benefits regardless of e-cigarette health costs in both the United States and United Kingdom. Conversely, scenarios in which e-cigarette promotion leads to renormalization of cigarette smoking or e-cigarettes are used primarily by youth who never would have smoked showed net health harms across all e-cigarette health costs. In other scenarios, the net health effect varied on the basis of the health cost of e-cigarettes.
Conclusions and relevance: According to this analysis, widespread promotion of e-cigarettes may have a wide range of population-level health effects, depending on both e-cigarette health risks and patterns of use. Absent the primary effect of e-cigarette promotion being only to divert current or future conventional cigarette smokers to e-cigarette use, the current uncertainty about the health risks of e-cigarettes, increasing e-cigarette use among youth, and the varying health effects at different e-cigarette health costs suggest a potential for harm.
Conflict of interest statement
Figures

Comment in
-
e-Cigarettes--The Roles of Regulation and Clinicians.JAMA Intern Med. 2015 Oct;175(10):1603-4. doi: 10.1001/jamainternmed.2015.4436. JAMA Intern Med. 2015. PMID: 26322472 No abstract available.
References
-
- Office for National Statistics. [Accessed March 10, 2015];Adult Smoking Habits in Great Britain, 2013. 2014 Nov 25; http://www.ons.gov.uk/ons/dcp171778_386291.pdf.
-
- Action on Smoking and Health. [Accessed March 10, 2015];Use of electronic cigarettes (vapourisers) among adults in Great Britain. 2015 May; http://www.ash.org.uk/files/documents/ASH_891.pdf.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
