

Ex vivo lung perfusion with adenosine A2A receptor agonist allows prolonged cold preservation of lungs donated after cardiac death
- PMID: 26323621
- PMCID: PMC4728036
- DOI: 10.1016/j.jtcvs.2015.07.075
Ex vivo lung perfusion with adenosine A2A receptor agonist allows prolonged cold preservation of lungs donated after cardiac death
Abstract
Objective: Ex vivo lung perfusion has been successful in the assessment of marginal donor lungs, including donation after cardiac death (DCD) donor lungs. Ex vivo lung perfusion also represents a unique platform for targeted drug delivery. We sought to determine whether ischemia-reperfusion injury would be decreased after transplantation of DCD donor lungs subjected to prolonged cold preservation and treated with an adenosine A2A receptor agonist during ex vivo lung perfusion.
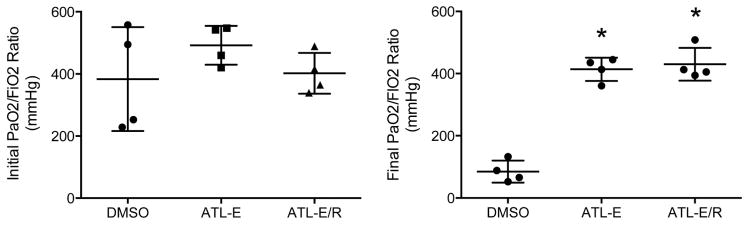
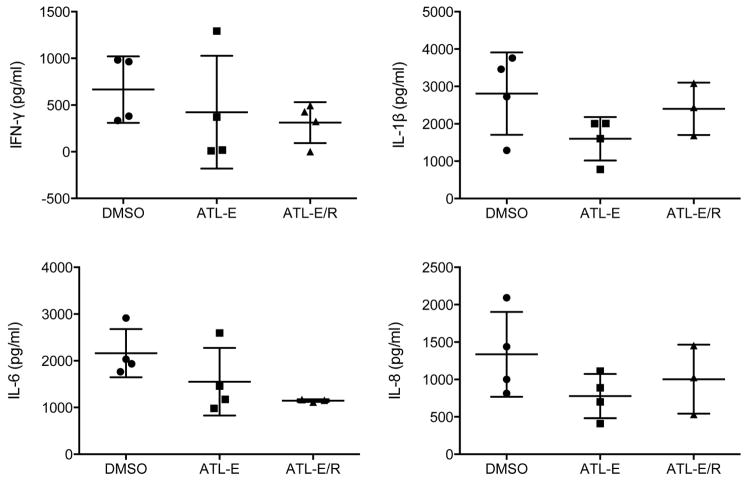
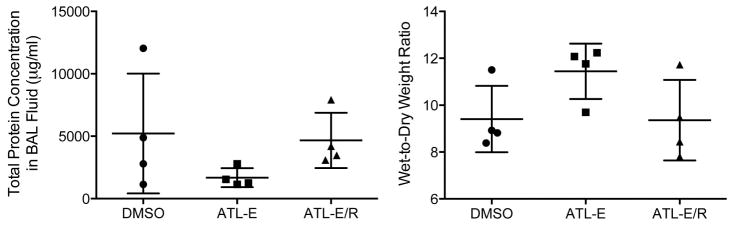
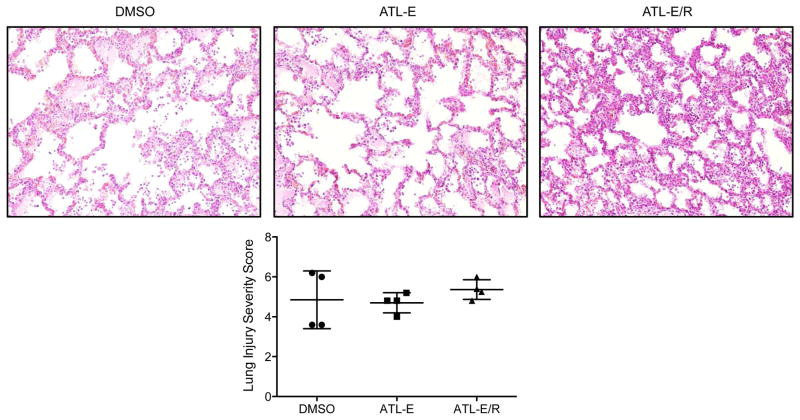
Methods: Porcine DCD donor lungs were preserved at 4°C for 12 hours and underwent ex vivo lung perfusion for 4 hours. Left lungs were then transplanted and reperfused for 4 hours. Three groups (n = 4/group) were randomized according to treatment with the adenosine A2A receptor agonist ATL-1223 or the dimethyl sulfoxide vehicle: Infusion of dimethyl sulfoxide during ex vivo lung perfusion and reperfusion (DMSO), infusion of ATL-1223 during ex vivo lung perfusion and dimethyl sulfoxide during reperfusion (ATL-E), and infusion of ATL-1223 during ex vivo lung perfusion and reperfusion (ATL-E/R). Final Pao2/Fio2 ratios (arterial oxygen partial pressure/fraction of inspired oxygen) were determined from samples obtained from the left superior and inferior pulmonary veins.
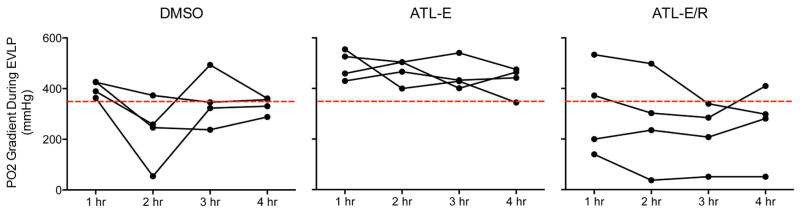
Results: Final Pao2/Fio2 ratios in the ATL-E/R group (430.1 ± 26.4 mm Hg) were similar to final Pao2/Fio2 ratios in the ATL-E group (413.6 ± 18.8 mm Hg), but both treated groups had significantly higher final Pao2/Fio2 ratios compared with the dimethyl sulfoxide group (84.8 ± 17.7 mm Hg). Low oxygenation gradients during ex vivo lung perfusion did not preclude superior oxygenation capacity during reperfusion.
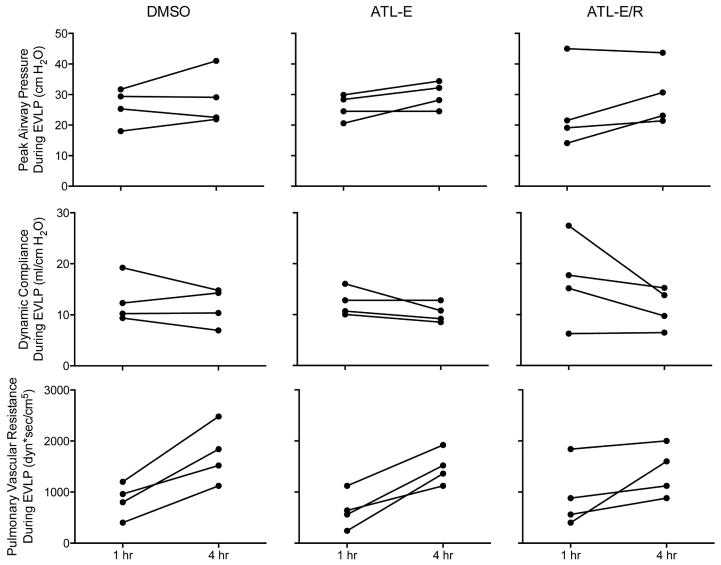
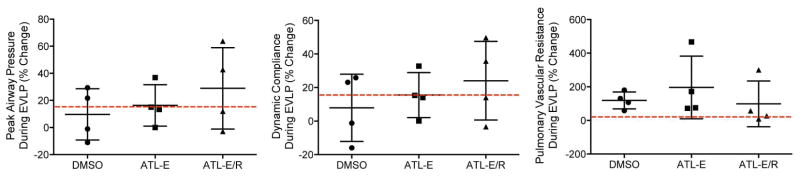
Conclusions: After prolonged cold preservation, treatment of DCD donor lungs with an adenosine A2A receptor agonist during ex vivo lung perfusion enabled Pao2/Fio2 ratios greater than 400 mm Hg after transplantation in a preclinical porcine model. Pulmonary function during ex vivo lung perfusion was not predictive of outcomes after transplantation.
Keywords: adenosine A2A receptor agonist; donation after cardiac death; ex vivo lung perfusion; lung transplantation; prolonged cold preservation.
Copyright © 2016 The American Association for Thoracic Surgery. Published by Elsevier Inc. All rights reserved.
Figures
Comment in
-
Discussion.J Thorac Cardiovasc Surg. 2016 Feb;151(2):546. doi: 10.1016/j.jtcvs.2015.07.084. Epub 2015 Aug 29. J Thorac Cardiovasc Surg. 2016. PMID: 26323623 No abstract available.
-
Ex vivo lung perfusion: The magic bullet to cure sick donor lungs?J Thorac Cardiovasc Surg. 2016 Feb;151(2):547-8. doi: 10.1016/j.jtcvs.2015.10.052. Epub 2015 Oct 23. J Thorac Cardiovasc Surg. 2016. PMID: 26806511 No abstract available.
References
-
- Cypel M, Keshavjee S. Strategies for safe donor expansion: donor management, donations after cardiac death, ex vivo lung perfusion. Curr Opin Organ Transplant. 2013;18:513–17. - PubMed
-
- Pierre AF, Sekine Y, Hutcheon MA, Waddell TK, Keshavjee SH. Marginal donor lungs: a reassessment. J Thorac Cardiovasc Surg. 2002;123:421–8. - PubMed
-
- Botha P, Trivedi D, Weir CJ, Searl CP, Corris PA, Dark JH, Schueler SV. Extended donor criteria in lung transplantation: impact on organ allocation. J Thorac Cardiovasc Surg. 2006;131:1154–60. - PubMed
-
- King RC, Binns OA, Rodriguez F, Kanithanon RC, Daniel TM, Spotnitz WD, Tribble CG, Kron IL. Reperfusion injury significantly impacts clinical outcome after pulmonary transplantation. Ann Thorac Surg. 2000;69:1681–5. - PubMed
-
- Christie JD, Sager JS, Kimmel SE, Ahya VN, Gaughan C, Blumenthal NP, Kotloff RM. Impact of primary graft failure on outcomes following lung transplantation. Chest. 2005;127:161–65. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
